![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
The adjective psychedelic in psychedelic
drugs comes from the Greek words
psyche ("mind") and delos ("clear, manifest, revealing"). The word
was coined in 1956 by Humphry Osmond, a psychiatrist who was
interested in hallucinogenic drugs as laboratory models of
schizophrenia. It was Osmond who supplied Aldoux
Huxley with the mescaline that inspired Huxley's classic
book, The Doors of Perception (1954).
Previously, psychiatrists had classified mescaline and LSD
as psychotomimetic drugs (mimicking psychosis) or hallucinogenics
(also with connotations of mental illness). Huxley was
looking for something more positive, and proposed the term phanerothyme,
from the Greek phanein (to reveal) and thymos
(soul). Humphrey countered with psychedelic,
from the Greek psyche (mind) and deloun (to
make manifest), and the latter term stuck.
Osmond also co-authored Models of Madness, Models of Medicine (1966, with Miriam Siegler), whose sociological interpretation of the "medical model" of psychopathology I teach in my introductory course
Legal restrictions on the availability of psychedelic drugs to researchers, as well ethical and legal restrictions on researchers, have effectively prevented much research on these "consciousness altering" substances from being conducted. Moreover, the environment in which such research has been conducted has been distorted by the "recreational" use of many of these substances, such as marijuana and LSD. Because most of the available research on the mental (as opposed to physiological) effects of psychedelic drugs is impressionistic and anecdotal, they did not get much attention in this course. But in the 2010s, with the trend toward legalization of marijuana and other psychedelic drugs for medical and recreational use picking up steam, it seemed that some actual research might get conducted, and so it seemed appropriate to fill out the story.
Classification of Psychoactive Drugs
 William Farthing,
whose Psychology of Consciousness (1992) offers as good a summary of research on
psychedelics, up to its publication date (and there hasn't much after that, until
lately), as can be found anywhere,
offers a useful classification
of psychoactive drugs. There
have been lots more added since
1992, which is a tribute, I guess, to the genius of
the recreational drug industry -- especially with
the increasing legalization of
marijuana. I don't intend to provide
comprehensive coverage of al of these drugs.
This isn't
a course on biochemistry or
pharmacology. If you're
really interested in the full range of psychoactive
drugs, and how they work in the
nervous system, I highly recommend "Drugs and the Brain" (Molecular
& Cell Biology 62, cross-listed as
Psychology 119 and Letters & Science 30) taught by
UCB's
Dr. David Presti -- one of Berkeley's most popular and
distinguished teachers.
William Farthing,
whose Psychology of Consciousness (1992) offers as good a summary of research on
psychedelics, up to its publication date (and there hasn't much after that, until
lately), as can be found anywhere,
offers a useful classification
of psychoactive drugs. There
have been lots more added since
1992, which is a tribute, I guess, to the genius of
the recreational drug industry -- especially with
the increasing legalization of
marijuana. I don't intend to provide
comprehensive coverage of al of these drugs.
This isn't
a course on biochemistry or
pharmacology. If you're
really interested in the full range of psychoactive
drugs, and how they work in the
nervous system, I highly recommend "Drugs and the Brain" (Molecular
& Cell Biology 62, cross-listed as
Psychology 119 and Letters & Science 30) taught by
UCB's
Dr. David Presti -- one of Berkeley's most popular and
distinguished teachers.
The distinction between "major" and "minor"
psychedelics was introduced by Charles Tart (1972), based
the degree to which the subjective effects of the drug are
under volitional control. on the amount ofvolitional
control which
The modern history of consciousness-altering drugs properly begins with Humphrey Davy, the English chemist who, as discussed in the lectures on Anesthesia and Coma, experimented with nitrous oxide (NO2) in the late 18th century. Davy did not pursue the anesthetic effects of nitrous, but he certainly appreciated its effects on consciousness:
"a thrilling all over me most exquisitely pleasurable.... The objects around me became dazzling, and my hearing more acute".
Davy's enthusiasm was infectious, as it were, and pretty soon the English "smart set" was holding regular nitrous oxide parties in which people -- for want of a better term -- got high. Later, after Morton's introduction of ether as a surgical anesthetic, ether parties were added to the social calendar.
The story of Davy's adventures with nitrous oxide are detailed by Richard Holmes in The Age of Wonder: How the Romantic Generation Discovered the Beauty and Terror of Science (2009), a history of the "second scientific revolution", of the late 18th and early 19th centuries. another view of Davy and the second scientific revolution is provided by Mike Jay in The Atmosphere of Heaven: The Unnatural Experiments of Dr. Beddoes and His Sons of Genius (also 2009).
 But
But  consciousness-altering
drugs have a more extended history than that. In fact,
they go back to the beginnings of Western civilization, with the
Oracle at Delphi, and her sister soothsayers (at left, image
from an cup, c. 440 BCE, showing King Aegeus of Athens and
Themis, the first Pythia, the earliest
surviving image of the Oracle of
Delphi; at right, a modern representation by John
Collier, 1850-1934, an English member of the "Pre-Raphaelite"
art movement). The Oracle held court
in the adyton, or forbidden inner
sanctum, of the Temple of Apollo
(the Greek god of prophecy) at Delphi, giving advice to private
and public figures. It was she, according to myth, who
prophesied that Oedipus
would kill his father and marry his mother. And it was
she who told Croesis, King of Lydia, that if he went to war
with Cyrus, King of the Persians, he would "destroy a great
empire" -- which he promptly did (his
own). According to legend (including Plutarch's Moralia,
c. 100 CE), the Oracle entered a trance
by breathing the vapors arising in the adyton from
a chasm in the earth, filtered through water from a sacred
spring. However, archaeological
excavations at Delphi conducted
around the turn of the century uncovered no such chasm, or any evidence of a natural gas that
could produce an intoxicated state. Later
geological analysis confirmed that Delphi was not
situated in the kind of volcanic
area that could produce such
gases. In the 1980s, however, Jelle
Zeilinga de Boer, a geologist at Wesleyan
University, and his colleagues, participating in
a new geological survey, discovered two fault
lines that intersected on Mount Parnassus, beneath the Temple of Apollo --
right at the site of the adyton.
One of the faults was marked by a series of
springs. Sampling the
water, they discovered traces of ethylene, a gas with a sweet odor
that is a known anesthetic agent. In
lighter doses, however, ethylene can induce a trance-like state
of delirium
characterized by euphoria, out-of-body
feelings, and amnesia.
consciousness-altering
drugs have a more extended history than that. In fact,
they go back to the beginnings of Western civilization, with the
Oracle at Delphi, and her sister soothsayers (at left, image
from an cup, c. 440 BCE, showing King Aegeus of Athens and
Themis, the first Pythia, the earliest
surviving image of the Oracle of
Delphi; at right, a modern representation by John
Collier, 1850-1934, an English member of the "Pre-Raphaelite"
art movement). The Oracle held court
in the adyton, or forbidden inner
sanctum, of the Temple of Apollo
(the Greek god of prophecy) at Delphi, giving advice to private
and public figures. It was she, according to myth, who
prophesied that Oedipus
would kill his father and marry his mother. And it was
she who told Croesis, King of Lydia, that if he went to war
with Cyrus, King of the Persians, he would "destroy a great
empire" -- which he promptly did (his
own). According to legend (including Plutarch's Moralia,
c. 100 CE), the Oracle entered a trance
by breathing the vapors arising in the adyton from
a chasm in the earth, filtered through water from a sacred
spring. However, archaeological
excavations at Delphi conducted
around the turn of the century uncovered no such chasm, or any evidence of a natural gas that
could produce an intoxicated state. Later
geological analysis confirmed that Delphi was not
situated in the kind of volcanic
area that could produce such
gases. In the 1980s, however, Jelle
Zeilinga de Boer, a geologist at Wesleyan
University, and his colleagues, participating in
a new geological survey, discovered two fault
lines that intersected on Mount Parnassus, beneath the Temple of Apollo --
right at the site of the adyton.
One of the faults was marked by a series of
springs. Sampling the
water, they discovered traces of ethylene, a gas with a sweet odor
that is a known anesthetic agent. In
lighter doses, however, ethylene can induce a trance-like state
of delirium
characterized by euphoria, out-of-body
feelings, and amnesia.
For more detail on the Oracle at Delphi, see "Questioning the Delphic Oracle" by John R. Hale, de Boer, and others, Scientific American, 8/2003.
For a discussion of ancient divination in general, including dream analysis and animal sacrifice as well as oracular pronouncements, see Divination and Human Nature: A Cognitive History of Intuition in Classical Antiquity (2016) by Peter Struck. Struck argues that ancient divination, in al its forms, more closely resembled what we would now call intuition, or maybe "gut instinct", as opposed to superstition and charlatanism.
A
little later, according to
Michael Pollan (in The
Botany of Desire: A Plant's-Eye
View of the World (2001), the Rig
Veda, one of the
earliest known religious texts
(dating from c. 1700-1100
BCE), took
soma, an intoxicant
probably related to the
mushroom Amanita muscaria, in order to
obtain knowledge of the devine
(Pollan is a professor
in the UCB School of
Journalism).
Also according to
Pollan, who read it in
Herodotus, the Scithyans, nomads living
north of the Black Sea in
the 8th century BCE, built
inhalers to trap the fumes
of burning cannabis buds,
after which
they would "rise up to dance and
betake themselves of
singing".
 And
finally, again according to
Pollan, Socrates, and Plato, among other
ancient Greek philosophers,
all participated in the
Mysteries of Eleusis, in which
they consumed
a potion made of ergot,
which has a chemical
structure resembling that of
LSD. Pollan
speculates that Plato's
"supernatural
metaphysics", in which the
ideal forms of things
exist in a world existing
beyond our senses, might
have had its origins in
ergot intoxication --
though this doesn't
explain Aristotle's
insistence that the only
reality is the one we know
directly, through our
senses. (Plato's
the one pointing up, in this
segment of Raphael's
painting, The
School of Athens; Aristotle
is the one pointing down;
Socrates is in the painting, too,
though not in this portion
of it.)
And
finally, again according to
Pollan, Socrates, and Plato, among other
ancient Greek philosophers,
all participated in the
Mysteries of Eleusis, in which
they consumed
a potion made of ergot,
which has a chemical
structure resembling that of
LSD. Pollan
speculates that Plato's
"supernatural
metaphysics", in which the
ideal forms of things
exist in a world existing
beyond our senses, might
have had its origins in
ergot intoxication --
though this doesn't
explain Aristotle's
insistence that the only
reality is the one we know
directly, through our
senses. (Plato's
the one pointing up, in this
segment of Raphael's
painting, The
School of Athens; Aristotle
is the one pointing down;
Socrates is in the painting, too,
though not in this portion
of it.)
Fast-forward to the 19th century, hallucinogenic drugs were a staple of the Romantic movement. And not just Humphrey Davies's nitrous-oxide parties, either. Napoleon's army discovered hashish during the conquest of Egypt (which may explain why they shot the nose off the Sphinx), and brought it back to France. Baudelaire wrote an entire book, Artificial Paradises (1860) retailing his own experiences with the drug.
And,
of course, the
British got
opium from India
. The
English
romantics, for
their part,
consumed their
share of opium,
and some literary
critics have
suggested that
it played no
small role in
their
movement.
Samuel Taylor
Coleridge
became addicted
to opium
(taken in the
form of
laudanum, an
infusion of
opium and
brandy),
and it's
been suggested
that he wrote
his famous poem,
"Kubla Kahn --
or, a Vision
in a Dream: A
Fragment",
under its
influence.
It's
also been
suggested that
his idea of
"willing
suspension of
disbelief) was
opium-inspired.
Shelley and
Byron also
used opium,
though not
Wordsworth.
The British may have gotten their opium from India (and sold it to China, leading to the 19th-century Opium Wars), but the Indians may have gotten it from somewhere else. In "Opium's Human History" Natural History, 03/2019), Lucy Inglis, a historian, notes that the earliest traces of opium poppy have been found in a Neolithic site in the Jordan Valley, dated to 8-10,000 years ago, and the earliest evidence of the use of opium for narcotic and analgesic purposes comes from a Neolithic site in Spain. Opium poppy has been found in other Neolithic sites as well. Opium then gradually moved east, into Greece (both Minoan and Mycenaean pottery depicts people with poppy capsules, and Homer mentions poppy in both the Iliad and the Odyssey), Bronze Age Egypt and the rest of the Middle East (the Ebers Papyrus, dated to 1550 BCE, gives instructions for using opium to calm a fussy child).
Consciousness-Altering Drugs Before the Sixties Also
Psychonauts:
Drugs and the
Making of the
Modern Mind
(2023) by MIke
Jay, a
cultural
historian
(reviewed by
Clare Bucknell
in "High
Achievers", New
Yorker,
04/24-05/01/2023,
from which
this image is
drawn) -- also
in Jay's book
Emperors of
Dreams: Drugs
in the
Nineteenth
Century
(2000).
Jay points out
that of
mind-altering
substances
such as opium,
nitrous oxide,
and later
ether,
hashish, and
cocaine were
very popular
among the
English
Romantics. And
not just
poets: none
other than
William James,
looking here
very much like
a hippie out
of
Haight-Ashbury
in the
1960s.
And also
Sigmund Freud,
who did some
of the
earliest
medical
experiments on
cocaine: see
his
posthumously
published Cocaine
Papers
(1974), edited
by Robert Byck
and Freud's
own daughter,
Anna. Also
Psychonauts:
Drugs and the
Making of the
Modern Mind
(2023) by MIke
Jay, a
cultural
historian
(reviewed by
Clare Bucknell
in "High
Achievers", New
Yorker,
04/24-05/01/2023,
from which
this image is
drawn) -- also
in Jay's book
Emperors of
Dreams: Drugs
in the
Nineteenth
Century
(2000).
Jay points out
that of
mind-altering
substances
such as opium,
nitrous oxide,
and later
ether,
hashish, and
cocaine were
very popular
among the
English
Romantics. And
not just
poets: none
other than
William James,
looking here
very much like
a hippie out
of
Haight-Ashbury
in the
1960s.
And also
Sigmund Freud,
who did some
of the
earliest
medical
experiments on
cocaine: see
his
posthumously
published Cocaine
Papers
(1974), edited
by Robert Byck
and Freud's
own daughter,
Anna. |
 The
prime user of
opium among
British
Romantics was
Thomas
De
Quincey, a onetime
friend of Wordsworth,
Coleridge, and other English Lake
Poets, whose Confessions of an
Opium-Eater (1869)
documented his (and their)
quaffing of laudanum, and argued
that opium-induced
brain changes spurred his (and
their) creativity. Don't
try this at home! De
Quincey
became addicted to both opium
and alcohol, and
died a broken man (for a recent
biography of de Quincey, see Guilty
Thing: A Life of Thomas De
Quincey by Frances Wilson,
2016; also; also Thomas De
Quincey and the Cognitive
Unconscious by Markus Iseli,
2015) . Here's
an extract
(sorry) in which De
Quincey describes the effects of
the drug (punctuation original):
The
prime user of
opium among
British
Romantics was
Thomas
De
Quincey, a onetime
friend of Wordsworth,
Coleridge, and other English Lake
Poets, whose Confessions of an
Opium-Eater (1869)
documented his (and their)
quaffing of laudanum, and argued
that opium-induced
brain changes spurred his (and
their) creativity. Don't
try this at home! De
Quincey
became addicted to both opium
and alcohol, and
died a broken man (for a recent
biography of de Quincey, see Guilty
Thing: A Life of Thomas De
Quincey by Frances Wilson,
2016; also; also Thomas De
Quincey and the Cognitive
Unconscious by Markus Iseli,
2015) . Here's
an extract
(sorry) in which De
Quincey describes the effects of
the drug (punctuation original):
Heavens!... [W]hat an upheaving, from its lowest depths, of the inner spirit!... Here was a panacea... for all human woes: here was the secret of happiness, about which philosophers had disputed for so many ages, at once discovered: happiness might now be bought for a penny, and carried in the waistcoat pocket: portable ecstasies might be corked up in a pint bottle: and peace of mind could be sent down in gallons by the mail coach.
 Fast forward again 100
years, and Aldous Huxley, the author of Brave New World and
other novels, not to mention the
visionary Perennial Philosophy,
consumes 400 milligrams
of mescalin dissolved in a glass of water
and reports the results in The
Doors of Perception:
Fast forward again 100
years, and Aldous Huxley, the author of Brave New World and
other novels, not to mention the
visionary Perennial Philosophy,
consumes 400 milligrams
of mescalin dissolved in a glass of water
and reports the results in The
Doors of Perception:
From what I had read of the mescalin experience I was convinced in advance that the drug would admit me, at least for a few hours, into the kind of inner world described by Blake and AE. But what I had expected did not happen. I had expected to lie with my eyes shut, looking at visions of manycolored geometries, of animated architectures, rich with gems and fabulously lovely, of landscapes with heroic figures, of symbolic dramas trembling perpetually on the verge of the ultimate revelation. But I had not reckoned, it was evident, with the idiosyncrasies of my mental make-up, the facts of my temperament, training and habits....
The change which actually took place in that world was in no sense revolutionary. Half an hour after swallowing the drug I became aware of a slow dance of golden lights. A little later there were sumptuous red surfaces swelling and expanding from bright nodes of energy that vibrated with a continuously changing, patterned life. At another time the closing of my eyes revealed a complex of gray structures, within which pale bluish spheres kept emerging into intense solidity and, having emerged, would slide noiselessly upwards, out of sight. But at no time were there faces or forms of men or animals. I saw no landscapes, no enormous spaces, no magical growth and metamorphosis of buildings, nothing remotely like a drama or a parable. The other world to which mescalin admitted me was not the world of visions; it existed out there, in what I could see with my eyes open. The great change was in the realm of objective fact. What had happened to my subjective universe was relatively unimportant. I took my pill at eleven. An hour and a half later, I was sitting in my study, looking intently at a small glass vase. The vase contained only three flowers-a full-blown Belie of Portugal rose, shell pink with a hint at every petal's base of a hotter, flamier hue; a large magenta and cream-colored carnation; and, pale purple at the end of its broken stalk, the bold heraldic blossom of an iris. Fortuitous and provisional, the little nosegay broke all the rules of traditional good taste. At breakfast that morning I had been struck by the lively dissonance of its colors. But that was no longer the point. I was not looking now at an unusual flower arrangement. I was seeing what Adam had seen on the morning of his creation-the miracle, moment by moment, of naked existence.
"Is it agreeable?" somebody asked. (During this Part of the experiment, all conversations were recorded on a dictating machine, and it has been possible for me to refresh my memory of what was said.)
"Neither agreeable nor disagreeable," I answered. "it just is."
***
Reflecting on my experience, I find myself agreeing ... with Broad "that the function of the brain and nervous system and sense organs is in the main eliminative and not productive. Each person is at each moment capable of remembering all that has ever happened to him and of perceiving everything that is happening everywhere in the universe. The function of the brain and nervous system is to protect us from being overwhelmed and confused by this mass of largely useless and irrelevant knowledge, by shutting out most of what we should otherwise perceive or remember at any moment, and leaving only that very small and special selection which is likely to be practically useful." According to such a theory, each one of us is potentially Mind at Large.... To make biological survival possible, Mind at Large has to be funneled through the reducing valve of the brain and nervous system. What comes out at the other end is a measly trickle of the kind of consciousness which will help us to stay alive on the surface of this Particular planet.... Most people, most of the time, know only what comes through the reducing valve and is consecrated as genuinely real by the local language. Certain persons, however, seem to be born with a kind of by-pass that circumvents the reducing valve. In others temporary by-passes may be acquired either spontaneously, or as the result of deliberate "spiritual exercises," or through hypnosis, or by means of drugs. Through these permanent or temporary by-passes there flows, not indeed the perception "of everything that is happening everywhere in the universe" (for the by-pass does not abolish the reducing valve, which still excludes the total content of Mind at Large), but something more than, and above all something different from, the carefully selected utilitarian material which our narrowed, individual minds regard as a complete, or at least sufficient, picture of reality.
The brain is provided with a number of enzyme systems which serve to co-ordinate its workings. Some of these enzymes regulate the supply of glucose to the brain cells. Mescalin inhibits the production of these enzymes and thus lowers the amount of glucose available to an organ that is in constant need of sugar. When mescalin reduces the brain's normal ration of sugar what happens? Too few cases have been observed, and therefore a comprehensive answer cannot yet be given. But what happens to the majority of the few who have taken mescalin under supervision can be summarized as follows.
The ability to remember and to "think straight" is little if at all reduced. (Listening to the recordings of my conversation under the influence of the drug, I cannot discover that I was then any stupider than I am at ordinary times.)
Visual impressions are greatly intensified and the eye recovers some of the perceptual innocence of childhood, when the sensum was not immediately and automatically subordinated to the concept. Interest in space is diminished and interest in time falls almost to zero.
Though the intellect remains unimpaired and though perception is enormously improved, the will suffers a profound change for the worse. The mescalin taker sees no reason for doing anything in particular and finds most of the causes for which, at ordinary times, he was prepared to act and suffer, profoundly uninteresting. He can't be bothered with them, for the good reason that he has better things to think about.
These better things may be experienced (as I experienced them) "out there," or "in here," or in both worlds, the inner and the outer, simultaneously or successively. That they are better seems to be self-evident to all mescalin takers who come to the drug with a sound liver and an untroubled mind.
These effects of mescalin are the sort of effects you could expect to follow the administration of a drug having the power to impair the efficiency of the cerebral reducing valve. When the brain runs out of sugar, the undernourished ego grows weak, can't be bothered to undertake the necessary chores, and loses all interest in those spatial and temporal relationships which mean so much to an organism bent on getting on in the world. As Mind at Large seeps past the no longer watertight valve, all kinds of biologically useless things start to happen. In some cases there may be extra-sensory perceptions. Other persons discover a world of visionary beauty. To others again is revealed the glory, the infinite value and meaningfulness of naked existence, of the given, unconceptualized event. In the final stage of egolessness there is an "obscure knowledge" that All is in all - that All is actually each. This is as near, I take it, as a finite mind can ever come to "perceiving everything that is happening everywhere in the universe."
 And a little later to
the era of modern jazz
and Beat poetry, here's Allen Ginsberg writing in the Atlantic
Monthly (August 1966), in favor of
the decriminalization of marijuana:
And a little later to
the era of modern jazz
and Beat poetry, here's Allen Ginsberg writing in the Atlantic
Monthly (August 1966), in favor of
the decriminalization of marijuana:
How much there is to be revealed about marijuana in this decade in America for the general public! The actual experience of the smoked herb has been clouded by a fog of dirty language perpetrated by a crowd of fakers who have not had the experience and yet insist on downgrading it. The paradoxical key to this bizarre impasse of awareness is precisely that the marijuana consciousness is one that, ever so gently, shifts the center of attention from habitual shallow, purely verbal guidelines and repetitive secondhand ideological interpretations of experience to more direct, slower, absorbing, occasionally microscopically minute engagement with sensing phenomena.
A few people don't like the experience and report back to the language world that it's a drag. But the vast majority all over the world who have smoked the several breaths necessary to feel the effect, adjust to the strangely familiar sensation of Time slow-down, and explore this new space thru natural curiosity, report that it's a useful area of mind-consciousness to be familiar with. Marijuana is a metaphysical herb less habituating than tobacco, whose smoke is no more disruptive than Insight.
And here's Ginsberg again, from an interview in the Paris Review (1965):
I smoked a lot of marijuana and went to the basement of the Museum of Modern Art in New York and looked at his water colors and that's where I began really turning on to space in Cezanne and the way he built it up... . I suddenly got a strange shuddering impression looking at his canvases, partly the effect when someone pulls a Venetian blind, reverses the Venetian -- there's a sudden shift, a flashing that you see in Cezanne canvases. Partly it's when the canvas opens up into three dimensions and looks like wooden objects, like solid-space objects, in three dimensions rather than flat. Partly it's the enormous spaces that open up in Cezanne's landscapes. And it's partly that mysterious quality around his figures.... They look like great huge 3-D wooden dolls, sometimes. Very uncanny thing, like a very mysterious thing -- in other words, there's a strange sensation that one gets, looking at his canvases, which I began to associate with the extraordinary sensation -- cosmic sensation, in fact -- that I had experienced catalyzed by Blake's "Sun-flower" and "Sick Rose" and a few other poems.... he produced a solid two-dimensional surface which when you looked into it, maybe from a slight distance with your eyes either unfocused or your eyelids lowered slightly, you could see a great three-dimensional opening, mysterious, stereoscopic, like going into a stereopticon.... Particularly there's one of rocks, I guess "Rocks at Garonne," and you look at them for a while, and after a while they seem like they're rocks, just the rock parts, you don't know where they are, whether they're on the ground or in the air or on top of a cliff, but then they seem to be floating in space like clouds, and then they seem to be also a bit like they're amorphous, like kneecaps or cockheads or faces without eyes. And it has a very mysterious impression. Well, that may have been the result of the pot. But it's a definite thing that I got from that.
 And finally, here's Carl Sagan, the
astronomer and science-popularizer, writing as "Mr. X" in Lester
Grinspoon's anthology, Marijuana Reconsidered (1969):
And finally, here's Carl Sagan, the
astronomer and science-popularizer, writing as "Mr. X" in Lester
Grinspoon's anthology, Marijuana Reconsidered (1969):
It all began about ten years ago. I had reached a considerably more relaxed period in my life -- a time when I had come to feel that there was more to living than science, a time of awakening of my social consciousness and amiability, a time when I was open to new experiences. I had become friendly with a group of people who occasionally smoked cannabis, irregularly, but with evident pleasure. Initially I was unwilling to partake, but the apparent euphoria that cannabis produced and the fact that there was no physiological addiction to the plant eventually persuaded me to try. My initial experiences were entirely disappointing; there was no effect at all, and I began to entertain a variety of hypotheses about cannabis being a placebo which worked by expectation and hyperventilation rather than by chemistry. After about five or six unsuccessful attempts, however, it happened. I was lying on my back in a friend's living room idly examining the pattern of shadows on the ceiling cast by a potted plant (not cannabis!). I suddenly realized that I was examining an intricately detailed miniature Volkswagen, distinctly outlined by the shadows. I was very skeptical at this perception, and tried to find inconsistencies between Volkswagens and what I viewed on the ceiling. But it was all there, down to hubcaps, license plate, chrome, and even the small handle used for opening the trunk. When I closed my eyes, I was stunned to find that there was a movie going on the inside of my eyelids. Flash... a simple country scene with red farmhouse, a blue sky, white clouds, yellow path meandering over green hills to the horizon. . . Flash... same scene, orange house, brown sky, red clouds, yellow path, violet fields... Flash... Flash... Flash. The flashes came about once a heartbeat. Each flash brought the same simple scene into view, but each time with a different set of colors... exquisitely deep hues, and astonishingly harmonious in their juxtaposition. Since then I have smoked occasionally and enjoyed it thoroughly. It amplifies torpid sensibilities and produces what to me are even more interesting effects.....
I can remember another early visual experience with cannabis, in which I viewed a candle flame and discovered in the heart of the flame, standing with magnificent indifference, the black-hatted and -cloaked Spanish gentleman who appears on the label of the Sandeman sherry bottle. Looking at fires when high, by the way, especially through one of those prism kaleidoscopes which image their surroundings, is an extraordinarily moving and beautiful experience.
I want to explain that at no time did I think these things 'really' were out there. I knew there was no Volkswagen on the ceiling and there was no Sandeman salamander man in the flame. I don't feel any contradiction in these experiences. There's a part of me making, creating the perceptions which in everyday life would be bizarre; there's another part of me which is a kind of observer. About half of the pleasure comes from the observer-part appreciating the work of the creator-part. I smile, or sometimes even laugh out loud at the pictures on the insides of my eyelids. In this sense, I suppose cannabis is psychotomimetic, but I find none of the panic or terror that accompanies some psychoses. Possibly this is because I know it's my own trip, and that I can come down rapidly any time I want to.
Given these kinds of reports, you would think that when the consciousness revolution hit in the 1960s, and again later in the 1980s, that the effects of marijuana, LSD, and other psychedelic drugs would have been the subject of intense research activity. But it was not to be. In the first place, as with Humphrey Davy's experience with nitrous oxide, people -- including researchers, like Timothy Leary and Richard Alpert -- were more interested in taking these drugs than in studying their effects. But second, and most important, government drug policy got in the way. In the Controlled Substances Act of 1970, both marijuana and LSD, along with MDMA (known on the steet as "Ecstasy" or "Molly", and commonly used as a date-rape drug) and Psilocybin ("magic mushrooms") were put on "Schedule I", subject to the most stringent regulations by the Drug Enforcement Administration (DEA), as drugs with the "no currently accepted medical use and a high potential for abuse". This effectively drove the drugs underground, and effectively precluded any basic or clinical research on their effects. And so the situation remains today -- at least so far as federal policy is concerned.
Most recently, however, state-level movements toward legalization, first in Colorado and Washington State, legalized the use of marijuana for either medical or recreational use. California already permits medical marijuana, and Proposition 64, legalizing recreational marijuana, was put on the ballot in 2016. For the record, I haven't smoked marijuana, or done anything else with it, for more than 35 years, and even then, like Bill Clinton, I didn't inhale (no wonder it had little effect on me!). I support legalization in principle -- recreational marijuana strikes me as no different from recreational alcohol -- but voted against Prop 64 because there are as yet no established standards for "driving under the influence" of the drug.
Which brings me to the subject of Maureen Dowd, an Op-Ed columnist for the New York Times, who sampled a little too much marijuana-laced candy which she bought at a Colorado dispensary after the state legalized the sale of the drug for recreational purposes (link to the article from the Times. 06/03/2014):
For an hour, I felt nothing. I figured I'd order dinner from room service and return to my more mundane drugs of choice, chardonnay and mediocre-movies-on-demand.
But then I felt a scary shudder go through my body and brain. I barely made it from the desk to the bed, where I lay curled up in a hallucinatory state for the next eight hours. I was thirsty but couldn't move to get water. Or even turn off the lights. I was panting and paranoid, sure that when the room-service waiter knocked and I didn't answer, he'd call the police and have me arrested for being unable to handle my candy.
I strained to remember where I was or even what I was wearing, touching my green corduroy jeans and staring at the exposed-brick wall. As my paranoia deepened, I became convinced that I had died and no one was telling me.It took all night before it began to wear off, distressingly slowly. The next day, a medical consultant at an edibles plant where I was conducting an interview mentioned that candy bars like that are supposed to be cut into 16 pieces for novices; but that recommendation hadn't been on the label.
The availability of private research funding, through such organizations as the Multidisciplinary Association for Psychedelic Studies, has allowed some research to go forward, but the federal restrictions still hamper the publication of this research and its translation into therapeutic uses. Anyway, almost all of this research is directed toward clinical applications, such as the use of marijuana or LSD in the treatment of anxiety or PTSD, or the relief of pain in chronically or terminally ill patients -- not on the alterations in consciousness that are the principal topic of this course.
Moving into the modern era of drug research, we begin with a number of drug-induced states that have been subject to careful experimental research. While not "psychedelic" in nature, these drugs do have effects on consciousness -- especially conscious memory. Much of this literature has its origins in the study of state-dependent learning (SDL) or state-dependent memory (SDM), an experimental paradigm in which an animal or human subject learns while under the influence of a drug (or not), and then is tested for retention of that learning while under the influence of a drug (or not). When learning condition (drug vs. no drug) is crossed with test condition (drug vs. no drug), the typical finding is of a statistical interaction: retention is best when the condition of test is the same as the condition of learning: drug-drug (D-D) or no-drug-no-drug (ND-ND)). Typically, there are also main effects, such that the drug impairs learning and retrieval. Typically, retention is best when both learning and test take place in the no-drug state.
The design for a basic SDL experiment takes the form of a 2x2 table:
Learning Trials |
Test Trials |
|
No Drug |
Drug |
|
No Drug |
+++ |
- |
Drug |
- |
++ |
Learning is best when both the acquisition and test trials take place in the non-drugged state. This is because SDL is induced by psychoactive drugs and, as a rule, psychoactive drugs tend to impair performance at both the encoding and retrieval stages of learning and memory (the stimulant Ritalin is an exception, but only in subjects with attention-deficit hyperactivity disorder). But otherwise, memory is actually best when the animal's physiological state at the time of test matches its state at the time of learning. The advantage of congruent over incongruent trials is the essence of state-dependent learning.
SDL was first noted by Girden and Culler (1937), in experiments on dogs who had been temporarily paralyzed by curare. These experiments were originally intended to examine the role of behavioral response in classical conditioning -- paralyzed animals can't make behavioral responses, so if they are capable of learning, they must be learning something other than the association of an environmental stimulus with a behavioral response. Of course, they're still able to make autonomic responses, such as heart-rate acceleration in response to a shock CS. Girden and Culler found that classical conditioning could be obtained in curarized dogs, but that the conditioned responses were stronger when the animals were still under the influence of the drug, and diminished after the drugs wore off. So, conditioned responses were, in some sense, conditional on the physiological state of the animal.
The first controlled studies of SDL were by Overton (1964), who studied rats trained to escape shock in a T maze. This research, done as Overton's doctoral dissertation, is now a classic of the animal-learning literature: the individual studies are masterpieces of experimental design. In his research, Overton trained rats to escape shock in a T-maze. During the acquisition phase, the animals were trained to turn left, or right, at the choice point in order to escape the shock (of course, the direction was counterbalanced across subjects). Then, learning was tested in a maze where escape was possible in either direction. Before training or testing, half the animals were given a (just barely) sub-anesthetic dose (amounting to 25 mg/kg) of sodium pentobarbital, a barbiturate sedative; training or testing took place after the animals had recovered somewhat from the initial dose, so that they were able to actually move through the maze!Overton did his research in the heyday of Skinnerian functional behaviorism, and so we was loathe to talk about his animals' internal states. Accordingly, he referred to his finding as a case of drug discrimination learning (DDL). That is, he considered the drug to be a discriminative stimulus, essentially controlling the animal's response. These days, we might say that the drug state signaled whether a left or right turn would be reinforced -- but even that is too mentalistic for some Skinnerians. Still, he argued that the total SDL observed in his experiments was simply an extreme form of drug discrimination learning.
The really interesting question, though, concerns conscious accessibility. Behind the notion of state-dependent learning is that the knowledge (e.g., about the maze and the contingencies of reinforcement) acquired during the drugged state is not consciously accessible during the non-drugged state, and vice-versa. This stance is compatible with the view of this course, which is that consciousness and conscious accessibility are issues to be taken seriously. But the whole question is anathema to a strict behaviorist, because mental states cannot enter into an explanation of behavior.
Since 1964 SDL (also known as drug discrimination learning) has been documented in a wide variety of nonhuman animal species, using a wide variety of drugs.Typically, SDL is studied in the milder form of drug discrimination learning. The higher doses of barbiturate that produce very dramatic SDL are potentially lethal -- and even when they're not, it's not a pleasant thing, for an experimenter to watch an animal stumble through a maze (and think what it's like for the animal). The lower doses employed in DDL have correspondingly less deleterious effects on the acquisition phase (remember, as a rule, psychoactive drugs impair both memory encoding and retrieval). Still, the assumption is that SDL and DDK represent different points on a single continuum of drug effects on memory.
Interestingly, SDL and DDL, viewed as "behavioral" preparations, have the usual pharmacological properties of the drugs that induce them:
Evidence of SDL is not restricted to dogs, rats, and other nonhuman animals. Human studies of state-dependent memory (SDM), paralleling animal studies of SDL, commonly make use of typical verbal-learning paradigms. In a typical experiment, a subject will study a word list in the D or ND state, and then attempt to remember that list in the same or opposite state. The general finding is that retention, typically measured by free recall, is best when there is a match between the conditions of encoding and retrieval. However, it should be noted that human studies typically do not yield the complete dissociations between D and ND states obtained in Overton's classic studies. Most likely, this is because ethical considerations preclude the use with humans of the very high, barely sub-lethal doses of anesthetics that Overton used with his rats. (And before you say anything, ethical considerations generally preclude the wanton use of such high doses with nonhuman animals as well -- which is why it's important that Overton's studies were so well controlled, so that they didn't have to be repeated unnecessarily to clean them up.
An early study by Swanson and Kinsbourne (1976) nicely illustrates the application of the SDM paradigm in humans. The subjects were "hyperactive" children, diagnosed with what we would now call attention deficit hyperactivity disorder (ADHD), who were being treated with the amphetamine Ritalin, a CNS stimulant that, paradoxically, has a beneficial effect in such patients (and is, essentially, the only exception t the general rule that psychoactive drugs impair cognitive performance). The children in the patient group were administered Ritalin either before breakfast or before lunch. At the doses employed, the drug takes effect in about 30 minutes, and lasts about 4 hours, permitting the children to be in the D and ND over the course of a single day. There was also a control group of children who had not been diagnosed with ADHD, but who, for the purposes of this experiment, were also run in the D and ND states. During the acquisition phase, the children performed a zoo location" task, essentially paired-associate learning, in which they were to assign each of 48 animal pictures to one of 4 cities.
On Day 1, the children learned 24 pairs in the D state, and 24 in ND. Errors in initial learning were reduced for the ADHD children who had received Ritalin; but performance was worse for the non-ADHD controls.
On Day 2, they relearned the same list, 12 D and 12 ND items from Day 1 in the D state, the remainder in ND, achieving the traditional 2x2 design. Errors in relearning were also reduced for the ADHD children, but increased for the normal controls. Most important, for the ADHD children, there was a symmetrical SDM effect. The ADHD children made more errors when the learning and relearning states were congruent. And the biggest effect was obtained in children for whom initial learning was helped by the drug.
A review by Eich (1980) documented SDM in humans with a wide variety of psychoactive drugs, especially anesthetic agents, amphetamine, alcohol, and marijuana. Apparently, any drug that acts on the central nervous system has the capacity to produce SDM in humans.
Eich's review also revealed
some interesting differences between the human and animal
studies.
Drug-induced SDM illustrates the encoding specificity principle in memory (ESP; Tulving & Thomson, 1973): memory is best when the cues provided at retrieval match those provided at the time of encoding. It also illustrates the effects of context on memory. The ESP is sometimes referred to as the principle of transfer-appropriate processing.
Encoding specificity, in
turn, is a variant on the cue-dependency principle
(Tulving, 1974). Although some memories occur to us
spontaneously, in general memory retrieval is prompted by
cues of various sorts, which contain information about the
target item to be remembered. The principle of
cue-dependency says simply that retrieval is best when
these cues are highly informative.
Mild to moderate doses of alcohol can lead to state-dependent memory, reflecting a change in consciousness between encoding and retrieval. But larger doses of alcohol can produce a lapse in consciousness itself.
In alcoholic blackout, a person carries out normal activities while intoxicated, but has no memory of them after sobering up. Blackout was authoritatively defined by Jellineck (1952), but it probably has been known to alcoholics since the beginning of alcoholism. It has also been formally recognized by the medical profession -- as in Bonhoeffer's reference to alcoholic palimpsests: a palimpsest being writing material, such as a piece of paper, from which previous writing has been erased. Goodwin et al. (1969) suggest that the term blackout is actually a corruption of blankout, an old printer's term for "pulling a blank", when a proof sheet comes out blank because of a failure to properly ink the galleys.
The occurrence of blackout marks the heightened sensitivity of the person to the effects of alcohol -- it occurs to non-alcoholics who have ingested very large amounts of alcohol, but it occurs to alcoholics even when they are only moderately intoxicated.
Ryback (1970) performed an in vivo study of blackouts with a group of inpatient alcoholics who, for research purposes, were housed in a special ward permitting controlled access to alcoholic beverages. After 1 week of enforced abstinence, they were permitted to drink at will for 1 week. Each morning, the patients were questioned about their memory for salient events of the previous day, and also about their experience of blackouts. Blackouts tended to occur following sudden, dramatic changes in blood alcohol levels.
There appear to be two
kinds of blackout.
Along these lines,
Washburne (1958) has noted two broad theoretical
approaches to alcoholic blackout.
Obviously, both theories could be right, but apply to blackouts at different stages of alcoholism. Most experimental evidence supports the characterization of blackout as reflecting encoding failure, or a failure to consolidate memory traces.
 Lisman (1974)
conducted a formal test of the state-dependency
hypothesis. Employing en in vivo setup like
Ryback's,
he put four chronic alcoholics, each with a history of
blackouts, through two cycles of 5 "dry" days followed by
7 "wet" days. Every afternoon he conducted a series
of memory tests, including recall of the previous day's events,
recognition of cards from Holtzman's version of Rorschach's inkblot
test, and paired-associate learning (a Chinese ideograph
paired with a color swatch). He also showed each
patient a picture of a room in the ward indicating the
location of a hidden bottle of alcohol. The results
yielded no evidence of state-dependency, even on the
hidden-bottle task. Generally, though, the
experiment provided good evidence of the encoding-failure
hypothesis. The patients had very poor memory for
the stimulus materials even after a 20-minute retention
interval, and memory after 20 minutes was a good predictor
of memory 24 hours later.
Lisman (1974)
conducted a formal test of the state-dependency
hypothesis. Employing en in vivo setup like
Ryback's,
he put four chronic alcoholics, each with a history of
blackouts, through two cycles of 5 "dry" days followed by
7 "wet" days. Every afternoon he conducted a series
of memory tests, including recall of the previous day's events,
recognition of cards from Holtzman's version of Rorschach's inkblot
test, and paired-associate learning (a Chinese ideograph
paired with a color swatch). He also showed each
patient a picture of a room in the ward indicating the
location of a hidden bottle of alcohol. The results
yielded no evidence of state-dependency, even on the
hidden-bottle task. Generally, though, the
experiment provided good evidence of the encoding-failure
hypothesis. The patients had very poor memory for
the stimulus materials even after a 20-minute retention
interval, and memory after 20 minutes was a good predictor
of memory 24 hours later.
While clinical lore has suggested that blackout might be a form of SDM, experimental studies suggest that the relevant memories are not accessible when the person becomes intoxicated again later. Rather, blackout appears to reflect a permanent encoding deficit, not unlike the anterograde the amnesia associated with bilateral damage to the medial temporal lobe memory system. This encoding deficit appears to be caused by rapidly rising levels of blood alcohol. All the evidence to date suggests that alcoholic blackout is an instance of anterograde amnesia. By virtue of a failure to properly encode memories, traces of experience are simply unavailable for retrieval.
However, it should be noted that almost all research on alcoholic blackout involves tests of explicit memory. It is possible that, like the amnesic syndrome, blackout impairs explicit memory but spares implicit memory. To date, however, there have been no studies testing for dissociations between explicit and implicit memory in alcoholic blackout. (Hint, hint.....)
A medically induced state
resembling alcoholic blackout is conscious sedation,
produced by various tranquilizing drugs:
As with general anesthesia, the mechanisms by which these drugs work is not well understood. However, their effects on memory are well known. All of these drugs can induce a dense anterograde amnesia covering the period during which the patient was sedated. As with the amnesic syndrome and alcoholic blackout, however, the patient remains conscious -- which is why it's called conscious sedation.
 This anterograde amnesia dissociates
explicit and implicit memory, impairing recall and
recognition, but spares priming. This may be
illustrated with a study by Cork et al. involving patients who
underwent outpatient surgery under conscious sedation with
propofol (trade name, Diprivan), a barbiturate-like synthetic
compound that is "unrelated to any other drug or class of
drugs". Introduced in 1985, propofol is widely used for
conscious sedation, and was the drug that, in overdose, killed
Michael Jackson, the "King of Pop". Following the same
sorts of procedures used to study implicit memory in general
anesthesia, Cork et al. employed a tape-recording consisting
of paired associates of the form ocean-water.
The tape was played continuously throughout the surgery, from
the first incision to the last stitch; another, matched set of
paired-associates served as a control. Memory was then
tested in the recovery unit.
This anterograde amnesia dissociates
explicit and implicit memory, impairing recall and
recognition, but spares priming. This may be
illustrated with a study by Cork et al. involving patients who
underwent outpatient surgery under conscious sedation with
propofol (trade name, Diprivan), a barbiturate-like synthetic
compound that is "unrelated to any other drug or class of
drugs". Introduced in 1985, propofol is widely used for
conscious sedation, and was the drug that, in overdose, killed
Michael Jackson, the "King of Pop". Following the same
sorts of procedures used to study implicit memory in general
anesthesia, Cork et al. employed a tape-recording consisting
of paired associates of the form ocean-water.
The tape was played continuously throughout the surgery, from
the first incision to the last stitch; another, matched set of
paired-associates served as a control. Memory was then
tested in the recovery unit.In the case of general anesthesia, spared priming counts as evidence of implicit perception, not just implicit memory, because adequately anesthetized patients have no conscious perceptual awareness of surgical events at the time they occur. In the case of conscious sedation, however, the patients are perceptually aware of the pairs as they were presented on the tape. They just forgot them later. Therefore, spared priming in conscious sedation counts as evidence of implicit perception.
In any event, it's now clear that both the major and the minor tranquilizers can impair consciousness. Patients have no conscious recollection of events that occurred during sedation, even though they retained "on line" conscious perception of those same events. But the memory impairment is not total: perceptual processing does leave some trace of the event in memory, and those implicit memories can still influence the patient's subsequent experience, thought, and action -- albeit outside awareness.
Interestingly, clinical lore holds that the same sedative drugs which produce amnesia in conscious sedation can also permit the recovery of memories which have been repressed or dissociated due to traumatic stress. Although this technique, known as narcosynthesis was popular during and after World War II, and remains in use even today, there is surprisingly little evidence that it actually works -- and, given is amnesic capacities, no reason to suppose it does. Mostly, though, the technique hasn't been subject to experimental study at all.
The use of barbiturates to recover traumatic memories was clearly influenced by Freud's psychodynamic theory -- though, in truth, it was Breuer and Freud's (1883-1885) pre-psychoanalytic hypothesis that "hysterics suffer from reminiscences" that really lies at the root of this practice. As recounted in the lectures on "'Hysteria' and Hypnosis", Breuer and Freud proposed that traumatic memories were repressed, and blocked from conscious awareness, but that hysterical symptoms symbolically represented the traumatic experience. Thus, they function as implicit memories of the repressed trauma. For Freud, at least in this early incarnation, the goal of treatment was to achieve abreaction, or conscious recall of the traumatic event, along with its accompanying emotion; and then catharsis, or a "purification" of the mind, leading to the restoration of mental health.
Of course, Freud had no evidence for this other than his own case studies. Nevertheless, this general therapeutic strategy of abreaction and catharsis was applied to the treatment of "war neurosis" (sometimes called "shell shock") during World War I. The general idea was that the traumatic experience of war caused amnesia by virtue of "psychogenic" processes of repression and dissociation, and that the unconscious traumatic memory caused the patient's symptoms -- of "hysterical" paralysis or whatever.
The only problem is that psychoanalysis takes a long time. In a military situation, it's necessary to achieve abreaction and catharsis quickly, so that the soldier can be returned to duty or discharged. For this purpose, Hadfield (1920) introduced hypnoanalysis, in which Freudian psychoanalysis was carried out while the patient was hypnotized. The general idea was that hypnosis was itself a form of regression, in which the patient had an "infantile" relationship with the hypnotist, and relied on a predominance of "primary process" thought. This characterization of hypnosis was wrong, but psychiatrists didn't know (or appreciate) that fact at the time. So, hypnoanalysis became quite popular, both in military medicine and in civilian clinics, for the treatment of hysterical patients who were, it was presumed, suffering from repressed "reminiscences" of past trauma.
But if psychoanalysis takes a long time, not every patient is hypnotizable, and so military and civilian psychiatrists sought a more reliable technique for speeding up psychoanalytic treatment. The answer was soon found in a new class of psychoactive drugs: the barbiturates, which had been first synthesized by a German researcher, Adolf von Bayer, in 1864 (he went on to found the pharmaceutical company that produces Bayer aspirin). Barbiturates, of course, depress cortical activity, and induce a sleep-like state of drowsiness -- which is pretty much what physicians thought hypnosis was at the time. Interestingly, the first psychological studies of the barbiturates by Lindemann (1932), found that they increased self-disclosure on the part of the subjects, who were apparently unable to resist answering even very personal questions. This observation is the origin of the label "truth serum" given to this class of drugs.
So it was only a short leap to the hypothesis that injecting a patient with barbiturates would enhance the psychoanalytic processes of abreaction and catharsis. And indeed, in short order Horseley (1936) developed "narco-hypnosis", and then "narco-analysis" for the purpose of facilitating the recovery of repressed traumas and forgotten childhood events.
Grinker and Spiegel (1943, 1945), still operating under the influence of Freudian psychodynamic theory, promoted the widespread use of barbiturates for the treatment of war neurosis (sometimes called "battle fatigue") in World War II. Patients would be given low dose via intravenous administration, and then receive suggestions that they relive whatever trauma they had experienced. They also introduced the term "narco-synthesis". In their psychoanalytically influenced view, it was not enough for the patient to relive his traumatic experience under the influence of the drug. It was also important that he transfer this memory to the non-drugged state, and integrate the experience, now accessible to conscious recollection, into his personality structure.
Grinker and Spiegel's use of narco-synthesis in the treatment of war neurosis is documented in "Let There Be Light", a propaganda film produced by John Ford, the famous Hollywood director. The film, once embargoed out of a fear that the public would turn against the war if they saw its psychological consequences for soldiers, has now been released on home video.
Grinker and Spiegel's apparent success in the treatment of war neurosis led to the widespread use of barbiturates in civilian psychiatry, as well. But it is important to understand that their "success" was only apparent. Rarely did they make any attempt to verify the memories recovered under the influence of the drug. Rather, they simply assumed that the recollections were valid. After all, they were vivid, detailed, and emotionally powerful; the memories made sense in the context of the patient's war experiences; and their drug-facilitated recovery led to symptom relief.
In fact, there has never been any controlled experimental or clinical study of "truth serum", with independent corroboration of the memories recovered thereby. There isn't even any study so simple as one that asks subjects to study a list of words, and after a delay long enough to induce forgetting, tests recall with and without administration of the drug. There's no question, as Lindemann originally observed, that sedated patients become more talkative - -that is, before they fall asleep. But this doesn't mean that their memories have improved.
A similar point can be made about the use of hypnotic suggestions for hypermnesia to recover repressed or dissociated - -or just plain forgotten -- memories. For details, see the lectures on "'Hysteria' and Hypnosis".
Nevertheless, the idea that "truth serum" (and, for that matter, hypnosis) works is very widespread. It is part of the clinical folklore shared by many psychotherapists and patients alike. And both techniques have been revived in contemporary practice, for the treatment of patients with post-traumatic stress disorder (PTSD). For example, barbiturates were used in the famous "Ramona" case in California, where a young woman recovered apparently false memories of childhood sexual abuse at the hands of her father -- leading to a huge and ugly lawsuit that shed light on the dangers of this practice. The practice of using drugs or hypnosis to recover ostensibly repressed or dissociated traumatic memories lacks any evidentiary basis. No scientific study backs the claims of practitioners who use these techniques.
In the absence of independent corroboration, no particular credence should be given to any memory recovered through the use of "truth serum", hypnotic hypermnesia, or any similar techniques.
Hallucinations
One of the major features of psychedelic
states are
hallucinations --false sensory/perceptual experiences that occur in the
absence of an adequate stimulus. Hallucinations are
similar to mental images, except that images are usually
experienced as voluntarily generated.
Hallucinations, by contrast, appear to occur
involuntarily, much like sensations and perceptions
derived from external stimuli.
Hallucinations, of course, are characteristic features
of "psychotic" forms of mental illness, such as
schizophrenia. Therefore, it is commonly assumed
that psychedelic states might serve as laboratory models
for understanding psychosis.
Perhaps the single most important clinical study of hallucinations, at least in the modern era, is Hallucinations by -- who else? --Oliver Sacks (2013; reviewed by Michael Greenberg in "The Hallucinators Among Us", New York Review of Books, 04/04/2013). Sacks himself suffers from migraine headaches (the subject of his first book, Migraine, originally published in 1970), whose auras include hallucinations; and, as he confesses in his book, he also experimented (a little) with psychedelic drugs as a medical student. So his study has the benefit of a first-person perspective on the subject. In his book, Sacks focuses on hallucinations that occur in the context of palpable brain insult, injury, or disease -- including, but not limited to, the temporary brain injury caused by the ingestion of psychedelic drugs. But he does not discuss the hallucinations associated with functional psychosis, such as schizophrenia or affective disorder. Sacks notes that psychotic hallucinations are dynamic, in that they address the patient (schizophrenic hallucinations are typically auditory, while the hallucinations associated with brain damage are typically visual), and the patient converses with the voices. In some way, psychotic hallucinations are related to the patient's personality and social circumstances; "organic" hallucinations are more impersonal and unemotional.
The "organic" hallucinations, including those produced by psychedelic drugs, are in some sense autonomous products of alternations in brain chemistry or activity. They also appear to be universal, in that their content seems not to vary by time, place, or person. Sacks and other neuroscientists sometimes call them proto-images, because they seem to consist of the building-blocks of more complex, personally significant images (think, perhaps, of Biederman's geons). As Sacks writes, "Such activity operates at a basic cellular level, are beneath the level of personal experience, The hallucinatory forms are, in this way, physiological universals of human experience".
Sacks asserts that more complex hallucinations emerge from higher levels of the visual system, including the temporal and parietal lobes, and are in some sense more specific and less universal -- tied to the patient's individual knowledge and memory. Possibly, these are the kinds of hallucinations noted by Wilder Penfield when he electrically stimulated various portions of the cortex prior to neurosurgery..
According to Sacks, synesthesia and phantom limbs also qualify as hallucinations.
Placebo Effects in Antidepressant Medications
Here there will be a summary of the
controversy surrounding Irving Kirsch's work, and
his claim that placebo effects
overwhelmingly account for the effects of antidepressant
drugs (Kirsch, 1998, 2002).
Whenever the effects of drugs on anything,
including consciousness, are discussed,
it's important to also discuss placebo effects. Every treatment -- not
just drugs, but also psychotherapy
and even surgery has a placebo component to it,
meaning that psychosocial factors, including "set
and setting" -- the context in which the
treatment is delivered and the subject's expectancies concerning the procedure, will affect the outcome
of the treatment.
I've
already discussed placebo effects on "The
Mysterious Leap from the Mind to the Body". In the standard definition
(Shapiro & Shapiro, 1997),
In clinical trials, placebos are typically used as controls to reveal whether new pharmacological agents actually have any specific effects on medical outcomes. In order to be approved by the US Food and Drug Administration, new drugs must be shown to be safe and effective -- the latter usually by comparison of the active drug to an inert placebo (the new treatment can also be compared to the current "standard of care". For more information, see "Understanding Clinical Trials" by Justin A. Zivin, Scientific American, 04/2000).
In the earlier lectures, I
discounted placebo effects on purely subjective states
as irrelevant to my analysis of the four problems of
mind and body. There, I was
interested in the effects of beliefs, expectations,
and the like on "bodily" states, such as heart rate
and blood pressure. (I had to discuss
placebos for pain because that's where most of the
placebo literature is; to
illustrate the issues involved). But because
the psychedelic states are induced by drugs, and all
drugs are assumed to have placebo components to them, placebo effects on
subjective mental states become relevant. Unfortunately, there
are relatively few studies comparing psychedelic
drugs to placebos, and placebo controls in
psychedelic drug research are problematic
anyway, for reasons I'll discuss later.
For the purposes of illustrating some of the issues, let's consider depression to be an altered state of consciousness -- which it is, once you think about it, even if we hardly ever think about that way.
In a provocative series of studies, Irving Kirsch and his associates (Kirsch & Sapirstein, 1998; Kirsch et al., 2002) have claimed that placebo effects accounted for as much as 75% of the effects of antidepressant drugs.
In a provocative article entitled "Listening to Prozac But Hearing Placebo", Kirsch & Sapirstein (Prevention & Treatment,1998) conducted a meta-analysis of 19 published studies in which an antidepressant medication (such as Prozac) was compared to placebo.On the basis of these results, K&S concluded that the active ingredients in antidepressant medications accounted for about 25% of the outcome in the drug treatment of depression; spontaneous remission (natural history) accounted for another 24%, and placebo accounted for approximately 51%.
As you might imagine, this claim drove
psychiatrists, who generally favor drugs over
psychotherapy, and even some psychologists (who
sometimes envy psychiatrists' ability to prescribe
drugs; ), quite crazy. Kirsch's title was, in fact, a
deliberate play on Listening to Prozac (1993), a pean to the drug by
psychiatrist Peter D. Kramer.
In response, Kirsch (Prevention
& Treatment, 1998a,
199b) compared the K&S meta-analysis to two
others, published at about the same time, which
used somewhat different
methods.
Kirsch concluded that "Inert placebos produce a powerful effect on depression", and "Antidepresant drugs enhance that effect to a relatively modest degree".
Still, there was the
possibility that the published studies
were somehow unrepresentative
of all the studies
conducted comparing
antidepressants and placebo.
Frankly, that possibility always
seemed unlikely, because you'd think
that, with the file-drawer
problem and all, the published
studies would be the best ones
available. But, in fact, there
were lots of unpublished studies
lying around. This is because
the Food and Drug
Administration, as part of its
protocol for approving new drugs,
requires only two
independent trials showing
that the investigational new
drug is significantly better
than placebo. In
principle, drug companies
could run dozens
or hundreds of trials, and
pick the two best to submit
for FDA approval. But
even those trials have to be
registered with the FDA in
advance. Accordingly, Kirsch et al. (Prevention
& Treatment, 2002)
made a Freedom of
Information Act to the FDA and obtained
the results of 47
randomized
placebo-controlled trials
for 6 different
antidepressants (38 of
these trials had data
suitable for their
analysis). Overall,
patients in the drug group
improved by 10.01 points
on the Hamilton
Rating Scale for Depression
(HAM_D), a commonly used
endpoint in treatment
studies; the comparable
figure for the patients
receiving
placebo was 7.82; put
another way, on average,
79% of the drug response
was duplicated by
placebo (unweighted
means from Table
2). That's
a significant difference,
which is why the drugs in
question received FDA
approval, For the drug
group. But Kirsch et
al., applying the FDA's
own standards for
evaluating new drugs,
concluded that "18% of
the drug response is
due to the
pharmacological
effects of the
medication".
This study, entitled "The Emperor's New Drugs", also drove the promoters of antidepressant medication crazy, all the more so because Kirsch followed up with a book, The Emperor's New Drugs: Exploding the Antidepressant Myth (2011). In response, Kramer recently published a new book, Ordinarily Well: The Case for Antidepressants (2016), which conceded that antidepressant medication works best for the most severely depressed patients, but argued that a combination of medication and psychotherapy is good for everyone.
The point of all this is not to diminish the value of antidepressants. Kirsch's data is convincing, but Kramer's response is probably correct: when people are depressed, the combination of drugs and psychotherapy can be very helpful. The point is that even powerful psychoactive drugs have substantial placebo components, and this is likely to be true for the major and minor psychedelics as well. As Kirsch et al. (2002) point out, "Placebo alcohol produces effects that are not observed when alcohol is administered surreptitiously...".
The "Gold Standard" for Drug TrialsIn principle,
assessing the effects of psychedelic drugs on
consciousness is no different from assessing drug
effects anywhere else in science or medicine.
There are standards, and these are embodied in the
procedure for a randomized, double-blind,
placebo-controlled drug trial. Unpack this
phrase, and you've got the whole methodology.
A major problem common
among studies using
the balanced placebo design is that investigators
often collapse across
conditions. For example, they
analyze pre-post changes in
performance for subjects who
were told they were
receiving THC, even though
half of them actually received
placebo. And they
analyze pre-post changes in
performance for subjects who received
THC, even
though half of them were
told they would receive
placebo. While this
design allows
investigators to analyze
the main effects of drug and
expectancy, what
we really want to see
are the interactions.
For example,
what changes
occurred in subjects
who received the drug,
but were told they
were receiving the
placebo; and in the
subjects who
were told they
were receiving
placebo, but who
actually received
the drug. This way, we can learn
how positive and negative
expectancies may moderate
the effects of the drug. And speaking of
"telling", another feature of
many alcohol studies is surreptitious
delivery, so that subjects
get alcohol but aren't told that's what they're
drinking. Supposedly,
this removes the "placebo"
component of alcohol
intoxication entirely.
But it's going
to be difficult
getting approval from a
"human subjects"
committee. |
|||||||||||
The term "minor psychedelics" refers mostly
to marijuana and its derivatives, such as hashish, whose
active ingredient is delta-9-tetrahydro-cannabinoid
(THC), found in the hemp plant cannabis
sativa). Marijuana and
hashish were introduced to Europe from Asia, Africa, and the Middle East, where
it had both medicinal and recreational uses.
Marijuana, came to the US via
Mexican guest workers, and it
1937 it was outlawed in the Marijuana Tax Act, and again in the Controlled
Substances Act of 1970 (which also outlawed the
major psychedelics, sucu as LSD and psilocybin).
In addition to "natural" marijuana, there is
also a synthetic marijuana, often blended with various
herbs and sold as K2. Although it is
typically marketed as incense, apparently everyone who
wants to know already knows that it's smokeable -- although
nobody knows precisely what hazards may be associated with
its use. Parents are largely ignorant of it, and it
doesn't
show up in conventional urine tests. The active
ingredients in K2 are synthetic cannabinoids, first
developed for research use by John W. Huffman, a chemist
at Clemson University, that mimic some of the psychedelic
effects of tetrahydrocannabinol (THC). Despite its
apparent availability at head shops everywhere, Huffman
never intended these synthetic cannabinoids for
non-research use, and as of 2010 their effects --
psychedelic and toxic -- have not been studied
formally. Nevertheless, K2 users show up in
emergency rooms with some frequency, complaining of
negative effects such as elevated physiological arousal
and attacks of paranoia. For this reason -- and
also, let's
face it, because it's
synthetic marijuana, some states have banned K2 and
similar drugs, although as of 2010 it isn't (yet)
listed on the DEA's
schedule of controlled substances.
For all the use it gets, and for all the attention paid to it in the legal and
policy domains, there has been surprisingly little research on
the psychological effects of marijuana. In his
comprehensive survey, LSD, Marijuana, Yoga, and Hypnosis,
Barber (1970) covered only three studies.
In the 1930s, New York's Mayor Fiorello LaGuardia commissioned a study of the drug, including a survey of its use and an experiment to document its effects (Mayor's committee, 1944). The report was published in 1944. The experiments were conducted with inmates of the city's jails, most of whom were already experienced users of marijuana.famous Riker's Island Prison. Unusually for the time, the experiment used a placebo control, but the study was not conducted double-blind, and the placebo was pretty transparent. In addition to documenting the subjective effects of smoking marijuana, the research found that even a relatively high dose of had little effect on simple mental functions, like simple reaction time. However, even a moderate dose had effects on complex functions, like complex reaction time. Whatever the effects, they were most obvious in subjects who had no previous experience with marijuana.
More than 20 years later, a study by
Clark & Nakashima (1968) confirmed many of these
findings with oral ingestion of
marijuana.
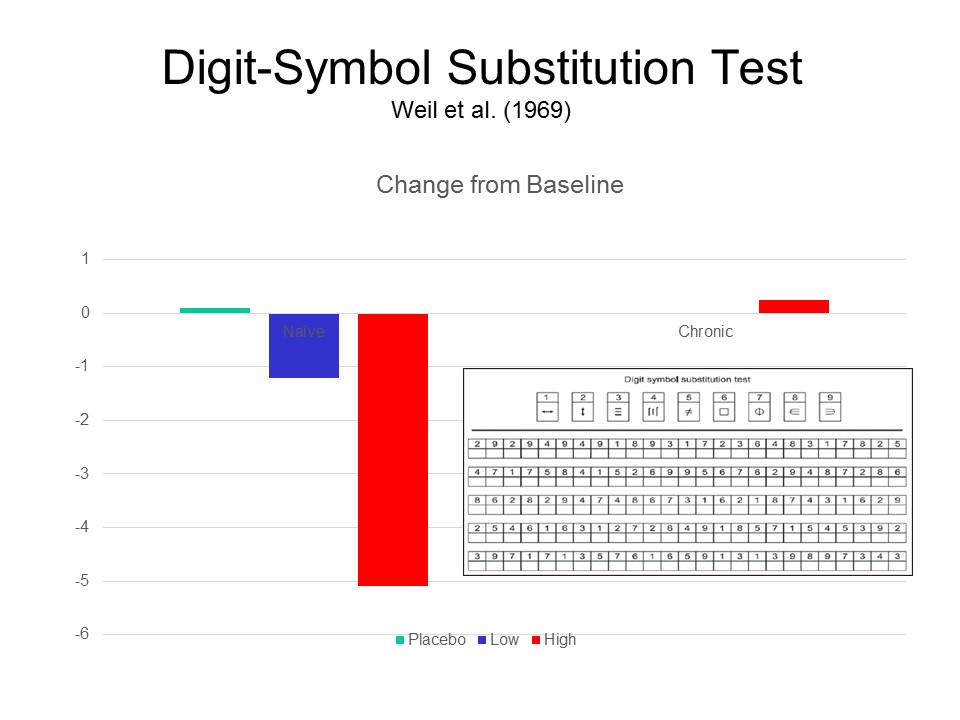 Weil
Weil  and his colleagues (Weil, Zinberg,
& Nelsen, 1968; Weil &
Zinberg, 1969) employed a true double-blind
procedure. Chronic and inexperienced
college students smoked 2
cigarettes containing a low or high dose
of THC (the chronic users were tested only with the
high dose, because they
experienced no subjective changes with the low
dose). Again, there were
dose-related decrements in performance on some
psychomotor tasks, especially
those of some complexity such
as digit-symbol substitution and pursuit-rotor
learning; but most of these effects were
confined to the inexperienced subjects.
and his colleagues (Weil, Zinberg,
& Nelsen, 1968; Weil &
Zinberg, 1969) employed a true double-blind
procedure. Chronic and inexperienced
college students smoked 2
cigarettes containing a low or high dose
of THC (the chronic users were tested only with the
high dose, because they
experienced no subjective changes with the low
dose). Again, there were
dose-related decrements in performance on some
psychomotor tasks, especially
those of some complexity such
as digit-symbol substitution and pursuit-rotor
learning; but most of these effects were
confined to the inexperienced subjects.
 The chief problem with the Weil study,
however, is that the double-blind placebo control failed. Only 15 minutes after smoking the joints, the
subjects were clearly able to recognize
whether they had been given the placebo
or the drug.
The chief problem with the Weil study,
however, is that the double-blind placebo control failed. Only 15 minutes after smoking the joints, the
subjects were clearly able to recognize
whether they had been given the placebo
or the drug.
This is a problem that will crop up later in studies of the major psychedelics, such as LS and psilocybin, and it may be insurmountable. The whole point of a double-blind placebo control is that neither the researchers nor the subjects can tell who has received the placebo. That works fine on the researchers' side: an independent pharmacist can pack capsules the drug or placebo, so that the researchers do not know which is which. And most drugs that have been subjected to double-blind placebo trials do not have immediate psychoactive effects (cancer drugs, for example, don't have any psychoactive effects; and antidepressants take a while to take effect); but psychedelic drugs have their effects on consciousness almost immediately. So subjects don't stay blind very long! In the case of psychedelics, as will be seen, researchers try to administer an "active" placebo, which mimics at least some of the psychological effects of the drug -- like nicotinic acid, which -- because it is the active ingredient of nicotine -- acts as a CNS stimulant. But even so, once subjects start hallucinating (because they've taken LSD) or fail to start hallucinating (because they've taken placebo), it's pretty easy to tell who's in which group.
 A study by Crancer
et al. (1969; see also Crancer, 1969; Kalant,
1969) compared the
effects of marijuana (1.7
grams) and alcohol (a 0.1
blood alcohol level) on performance on
a driving simulator over a period of 4-1/2
hours. The subjects had
prior experience with both marijuana
and alcohol. Alcohol impaired driving
performance, compared to a no-treatment control
group, but marijuana did not.
A study by Crancer
et al. (1969; see also Crancer, 1969; Kalant,
1969) compared the
effects of marijuana (1.7
grams) and alcohol (a 0.1
blood alcohol level) on performance on
a driving simulator over a period of 4-1/2
hours. The subjects had
prior experience with both marijuana
and alcohol. Alcohol impaired driving
performance, compared to a no-treatment control
group, but marijuana did not.
This is not to say that it's OK to drive after smoking marijuana. It probably isn't -- not least because, following legalization, the California Highway Patrol and other police agencies have announced that they will test suspicious drivers for THC, just as they now test subjects for blood-alcohol levels. Whether you're actually impaired or not, if you have high levels of THC or alcohol in your body, you're going to be in trouble.
 As
As 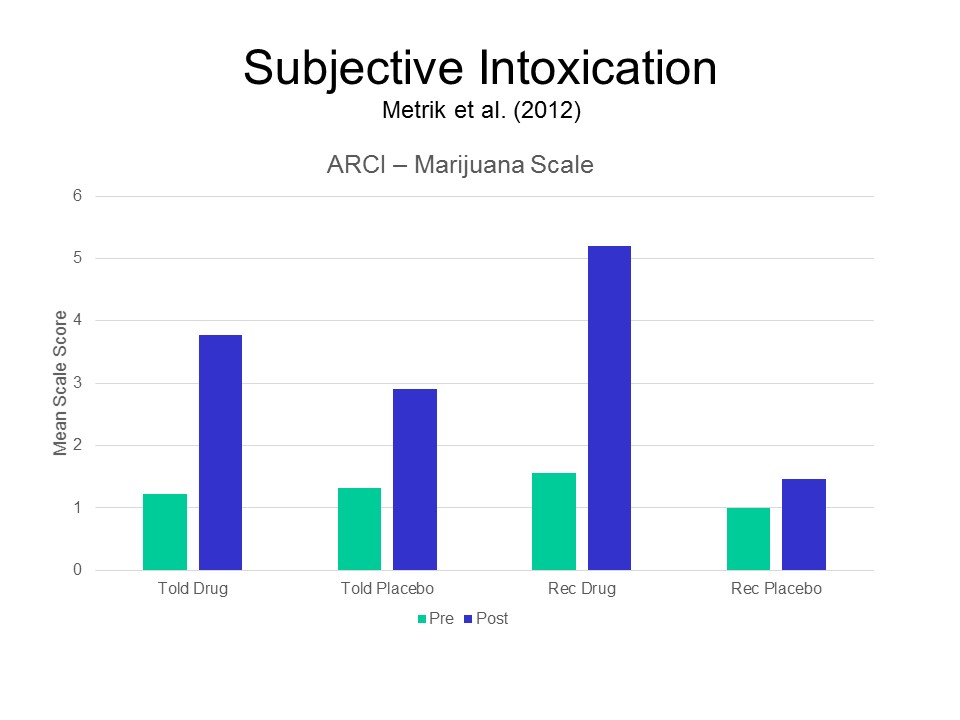 of 2016, only one study of
marijuana, by Matrik et al. (2012), has used the balanced
placebo design with college students who
already had some experience with marijuana. Recall that
in this design, some subjects are told they are getting the placebo, when they
really are getting the active drug. This condition
ostensibly "balances" the usual placebo
condition, in which subjects are led to expect
they are getting the drug, but are getting only an
inert substance. This is also one of the few
studies to assess alterations
in consciousness induced by
marijuana, as opposed to
changes in performance on
various psychomotor tasks - -though they
did that as well. The subjects were
college students, all
regular marijuana users, who received a
2.8% dose of THC or placebo.
Subjective "intoxication" was measured
by the Addiction Research Center
Inventory (ARCI), an
instrument designed
to assess the subjective effects of
all sorts of psychoactive drugs. The ARCI
contains a large number of items
charting effects on sensation and
perception,
bodily symptoms and processes,
and feelings and
attitudes. Unfortunately,
this study, like most using
the balanced-placebo design,
does not analyze these two
conditions separately, but you can
still get the idea:
subjects who smoked
marijuana, even those
who were told they
were getting placebo,
showed strong effects
of intoxication; those
who received placebo,
even those who were
told they were
getting marijuana,
felt little
subjective change. The
double-blind deception involved was fairly
successful, but 6% of
the subjects in the Told THC/Received
Placebo condition suspected that they
were not smoking real marijuana, and 21% of
the subjects in the Told Placebo/Received
THC condition suspected that they were
smoking the real thing.
of 2016, only one study of
marijuana, by Matrik et al. (2012), has used the balanced
placebo design with college students who
already had some experience with marijuana. Recall that
in this design, some subjects are told they are getting the placebo, when they
really are getting the active drug. This condition
ostensibly "balances" the usual placebo
condition, in which subjects are led to expect
they are getting the drug, but are getting only an
inert substance. This is also one of the few
studies to assess alterations
in consciousness induced by
marijuana, as opposed to
changes in performance on
various psychomotor tasks - -though they
did that as well. The subjects were
college students, all
regular marijuana users, who received a
2.8% dose of THC or placebo.
Subjective "intoxication" was measured
by the Addiction Research Center
Inventory (ARCI), an
instrument designed
to assess the subjective effects of
all sorts of psychoactive drugs. The ARCI
contains a large number of items
charting effects on sensation and
perception,
bodily symptoms and processes,
and feelings and
attitudes. Unfortunately,
this study, like most using
the balanced-placebo design,
does not analyze these two
conditions separately, but you can
still get the idea:
subjects who smoked
marijuana, even those
who were told they
were getting placebo,
showed strong effects
of intoxication; those
who received placebo,
even those who were
told they were
getting marijuana,
felt little
subjective change. The
double-blind deception involved was fairly
successful, but 6% of
the subjects in the Told THC/Received
Placebo condition suspected that they
were not smoking real marijuana, and 21% of
the subjects in the Told Placebo/Received
THC condition suspected that they were
smoking the real thing.
 The
Metrik et al. (2012) experiment was intended
to study the effects of marijuana
intoxication on various
aspects of impulsivity, employing a variety
of experimental tasks,
but yielding
mixed and confusing results.
The
Metrik et al. (2012) experiment was intended
to study the effects of marijuana
intoxication on various
aspects of impulsivity, employing a variety
of experimental tasks,
but yielding
mixed and confusing results.
On
the Stroop Interference Task, for example, subjects who smoked marijuana sowed a small increase in response latency, while those who were told they were getting the drug showed a larger reduction in response latency.
On
a "Stop-Signal" reaction time task, where subjects had to inhibit a dominant response, subjects who smoked marijuana showed a small increase in response latency, while those who received the placebo again showed a slight reduction.
Perhaps the best systematic description of the alterations in consciousness induced by marijuana was provided by Tart in On Being Stoned: the Subjective Effects of Marijuana Intoxication (1971), based on his survey of California college students who were experienced users of the drug. These changes include:
It's
important to point out, though, that these changes are not
necessarily experienced by first-time users of the drug.
There is a kind of "culture" to marijuana use, in which novices
are taught by mor experienced users what to expect, and what to
notice, about their experience (Carlin et al.,
1974).
Michael Pollan, in The Botany of
Desire (2001), has proposed that
there is an important link between the alterations of
consciousness experienced under marijuana and the
drug's
effects on "short-term" memory -- by which they
really mean long-term
memory. Remember, in
psychology, short-term memory
refers to memory that covers about
30 seconds of undistracted time after an event; long-term
memory refers to whatever
people remember of an event after
about 30 seconds of
distraction. Patient H.M.
was often characterized as having
a "short-term memory disorder",
but n fact his short-term memory
was reasonably intact. What
H.M. lacked was the capacity to
convert short-term memories into long-term
memories. He described
his own
memory as like awakening
from a dream" -- with memory
quickly slipping
away from him over
even a very short retention
interval.
 Here is
Pollan, inspired by Aldous
Huxley's
description of his experiences with
mescaline in The Doors of
Perception, writing
about marijuana (2001, pp. 159-162,
168-169, 170):
Here is
Pollan, inspired by Aldous
Huxley's
description of his experiences with
mescaline in The Doors of
Perception, writing
about marijuana (2001, pp. 159-162,
168-169, 170):
The scientists I spoke to were unanimous in citing short-term memory loss as one of the key neurological effects of the cannabinoids [based mostly on laboratory studies with nonhuman animals]. In their own way, so were the "poets" who tried to describe the experience of cannabis intoxication. All talk about the difficulty of reconstructing what happened mere seconds ago and what a Herculean challenge it becomes to follow the thread of a conversation (or a passage of prose) when one's short-term memory isn't operating normally.
At any given moment my senses present to my consciousness -- the perceiving "I" -- a blizzard of data no human mind can completely absorb.
The cannabinoid network [of neurons in the brain] appears to [vigilantly shift] the vast chaff of sense impression from the kernels of perception we need to remember if we're to get through the day and get done what needs to be done.
The THC in marijuana and the brain's endogenous cannabinoids work in much the same way, but THC is far stronger and more persistent than anandamide [an endogenous THC-like chemical, much like endorphin], which, like most neurotransmitters, is designed to break down very soon after its release....
What this suggests is that smoking marijuana may overstimulate the brain's built-in forgetting faculty, exaggerating its normal operations.
This is no small thing. Indeed, I would venture that, more than any other singe quality, it is the relentless moment-by-moment forgetting, this draining of the pool of sense-impression almost as quickly as it fills, that gives the experience of consciousness under marijuana its peculiar texture. It helps account for the sharpening of sensory perceptions, for the aura of profundity in which cannabis bathes the most ordinary insights, and, perhaps most important of all, for the sense that time has slowed or even stopped. For it is only by forgetting that we ever really drop the thread of time and approach the experience of living in the present moment, so elusive in ordinary hours. And the wonder of that experience, perhaps more than any other, seems to be at the very heart of the human desire to change consciousness, whether by means of drugs or any other technique....
Memory is the enemy of wonder, which abides nowhere else but in the present. This is why, unless you are a child, wonder depends on forgetting....
Ordinarily we think of drug experiences as additive -- it's often said that drugs "distort" normal perceptions and augment the data of the senses (adding hallucinations, say), but it may be that the very opposite is true -- that they work by subtracting some of the filters that consciousness normally interposes between us and the world.
This, at least, was Aldous Huxley's conclusion in The Doors of Perception.... In Huxley's view, [mescaline] disables what he called "the reducing valve" of consciousness, his name for the conscious mind's everyday editing faculty. The reducing valve keeps us from being crushed under the "pressure of reality", but it accomplishes this at a price, for the mechanism prevents us from ever seeing reality as it really is. The insight of mystics and artists flows from their special ability to switch off the mind's reducing valve. I'm not sure that any of us ever perceives reality "as it really is" (how would one know?), but Huxley is persuasive in depicting wonder as it happens when we succeed in suspending our customary verbal and conceptual ways of seeing....
So what happens under the influence of drugs or, for that matter, inspiration? In Huxley's metaphor, the reducing valve is opened wide to admit more of experience. This seems about right, though I'd qualify it by suggesting (as Huxley's own examples do) that the effect of altered consciousness is to admit a whole lot more information about a much smaller increment of experience....
The usual process by which the grains of perception pass us by slows way down, to the point where the conscious I can behold each grain in its turn, scrupulously examining it from every conceivable angle (sometimes from more angles that it even has), until all there is is the still still point at the hourglass's waist, where time itself appears to pause....
 Earlier, in the lecture
on "Meditation"
I suggested that there might be
something artificial about the attempt
to achieve nirvana though
artificial means like EEG alpha-wave
biofeedback. And, in fact, some
fundamentalist Christians have pointed
out that the Bible (both the Hebrew
Bible and the New Testament) prohibits
"sorcery" of all kinds, including the
use of drugs in an attempt to
communicate with, or divine knowledge
from, God.
Earlier, in the lecture
on "Meditation"
I suggested that there might be
something artificial about the attempt
to achieve nirvana though
artificial means like EEG alpha-wave
biofeedback. And, in fact, some
fundamentalist Christians have pointed
out that the Bible (both the Hebrew
Bible and the New Testament) prohibits
"sorcery" of all kinds, including the
use of drugs in an attempt to
communicate with, or divine knowledge
from, God.
Pollan has an answer to this, echoing
Huxley (2001, pp. 170-171):
Aldous Huxley did his best to argue us out of the view that a chemically conditioned spiritual experience is false -- and he did so long before we knew anything about cannabinoid or opioid receptor networks. "In one way or another, all our experiences are chemically conditioned, and if we imagine that some of them are purely 'spiritual', purely 'intellectual', purely 'aesthetic', it is merely because we have never troubled to investigate the internal chemical environment at the moment of their occurrence." He points out that mystics have always worked systematically to modify their brain chemistry, whether through fasting, self-flagellation, sleeplessness, hypnotic movement, or chanting.... What all this suggests is that the workings of consciousness are both more and less materialistic than we usually think: chemical reactions can induce thoughts, but thoughts can also induce chemical reactions.
The sad fact is that most of
the research on marijuana and memory has
been don on nonhuman animals. If I
were going to do research on marijuana and
consciousness, I'd start
where Huxley and Pollan started - -with
memory, examining the effects of the drug
on both "short-term" and "long-term"
memory, to determine
whether, indeed, marijuana
affects STM, and especially the transfer
from STM to LTM, and how any such changes
relate to the subjective effects of THC
intoxication.
"High Time" -- Editorial Series in the New York TimesIn July and
August 2014, the New York Times took a strong
editorial position favoring the legalization, or at
least the decriminalization, of marijuana. A
series of editorials examined the issue from all
sides. the series constitutes the best summary of
the current situation -- legal, medical, and social --
that I know. Links to the editorials, and the discussion that ensued, are provided in the list below. Of greatest relevance to this course is Philip Boffey's summary of the medical and scientific evidence about marijuana (#4 in the list above), which I summarize here:
|
 Mescaline,
psilocybin, LSD, and other "major psychedelics" have profound psychological effects, testifying
to the potency of the drugs involved. Even with these substances, however, the effects
on mental function are moderated by extraneous variables, such as the setting in which
the drug is taken (medical, research, or
recreational), the subjects "set"
or expectations (as in placebo effects), and the
personality of the subject (for a comprehensive review, see LSD,
Marijuana, Yoga, and Hypnosis by T.X. Barber, 1970).
Mescaline,
psilocybin, LSD, and other "major psychedelics" have profound psychological effects, testifying
to the potency of the drugs involved. Even with these substances, however, the effects
on mental function are moderated by extraneous variables, such as the setting in which
the drug is taken (medical, research, or
recreational), the subjects "set"
or expectations (as in placebo effects), and the
personality of the subject (for a comprehensive review, see LSD,
Marijuana, Yoga, and Hypnosis by T.X. Barber, 1970).
Mescaline was identified as the major ingredient in peyote by Heffter in 1896, though some claim that other substances in the peyote plant also contribute to the experience. Methoxyamphetamine is a much more powerful synthetic version of mescaline.
LSD was synthesized by Albert Hoffman in 1943, as an offshoot of his work for Sandoz, a Swiss pharmaceutical firm, on medical uses of the ergot fungus. Technically, it is LSD-25, referring to the 25th semisynthetic compound that Hoffman produced. In trials on laboratory animals, it appeared to be inert, but when Hoffman took some himself. Hoffman described his experiences as follows (quoted in Snyder, 1996):
Last Friday, April 16, 1943, I was forced to interrupt my work in the laboratory in the middle of the afternoon and proceed home, being affected by a remarkable restlessness combined with a slight dizziness. at home I lay down and sank into a not unpleasant intoxicated-like condition, characterized by an extremely stimulated imagination. In a dreamlike state with eyes closed I perceived an uninterrupted stream of fantastic pictures, extraordinary shapes with intense, kaleidoscopic play of colors. After some two hours this condition faded away.
On April 19, after taking merely 0.25 mg of LSD-25, which we now know to be a massive dose, Hoffman reported a more intense experience:
Everything in my field of vision wavered and was distorted as if seen in a curved mirror.... Pieces of furniture assumed grotesque, threatening forms.... The lady next door, whom I scarcely recognized,... was no longer Mrs. R. but rather a malevolent, insidious witch with a colored mask.... Even worse than the demonic transformations of the outer world were the alterations thta I perceived in myself, in my inner being. Every exertion of my will, every attempt to put an end to the disintegration of the outer world and the dissolution of my ego, seemed to be wasted effort. A demon had invaded me, had taken possession of my body, mind and soul. I jumped up and screamed, trying to free myself from him, but then sank down again and lay helpless on the sofa.... I was siezed by the dreadful fear of going insane. I was taken to another world, another place, another time. My body seemed to be without sensation, lifeless, strange. Was I dying? Was this the transition? At times I believed my self to be outside my body, and then perceived clearly, as an outside observer, the complete tragedy of my situation.... Would [my wife and three children] ever understand that I had not experimented thoughtlessly, irresponsibly, but rather with the utmost caution, and that such a result was in no way forseeable?
Sandoz thought that LSD might have uses in psychotherapy, and provied samples for free to researchers -- including, eventually, Timothy Leary and his colleagues at the Harvard Psilocybin Project. And the rest is history.
Psilocybin, is the active ingredient in so-called
"magic mushrooms", identified by Hoffman in
1958 (psilocyn is another). Hoffman's
self-experimentation convinced him that the
experience induced by psilocybin
was essentially the same as that induced by LSD --
if not as potent. Both ingredients have a
chemical structure very similar to the neurotransmitter serotonin.
Another herbal hallucinogen from the
shamanic tradition of Mexico is Salvia (salvia
divinorum), a member of the mint family (also
known as "diviner's sage", "Sally-D",
and "magic mint"). According to an article in
the New York Times ("Popularity of a
Hallucinogen May Thwart Its Medical Uses" by Kevin
Sack & Brent McDonald, 09/09/2008), Salvia has
emerged as a popular drug only in the last decade or
so, and there is so little literature on it that
even the US Drug Enforcement Agency has been unable
to decide whether to list it, like marijuana and
LSD, as a controlled substance. However, this
lack of scientific evidence has not prevented
several states, and several countries in Europe and
Asia, from banning or otherwise regulating the
substance. Salvia
is usually smoked, though it can also be chewed or
consumed in a tincture. According to the
article, "Users often report a sudden dissociation
from self, as if traveling through time. The
experience tends to be solitary, introspective and
sometimes fearful.... Regular users say it can
be a restorative, even spiritual tonic, and recall
their visualizations with precision". The
effects of even a small dose of salvia can be very
powerful, sometimes resembling the out-of-body
experience, and often quite unpleasant or
disturbing. Perhaps for this reason, online
sales often come with the caution to use it only
with a "sober sitter" in attendance. The active ingredient in Salvia, Salvinorin
A, stimulates only the kappa opioid
receptor in the brain, in contrast to LSD,
which may stimulate as many as 50 different
receptors. For this reason, it may constitute
a new class of psychedelic substance. As with
LSD and marijuana, there is some interest in its
potential medical uses, as in psychotherapy or pain
relief, but little research is available to date,
and most use appears to be recreational. As of
2009, the federal Drug Enforcement Administration
did not regulate Salvia, listing it only as a "drug
of interest", but a number of states list it as a
"Schedule 1" drug, along with LSD and Ecstasy.
As with all the other substances discussed here, Don't try this at home alone !
Research on LSD and
psilocybin in the United States began in 1949, soon after LSD was synthesized -- first as a
means of simulating psychosis, and then as a vehicle for
psychotherapy, especially as a treatment for
alcoholism. Although a large literature developed,
most of it was of poor quality, anecdotal or lacking in
essential controls. In the hands of the "Cambridge
Quartet" of psychedelic researchers -- Timothy Leary,
Richard Alpert (later known as Baba Ram Das), Huston Smith
(subsequently a professor of religious studies at UC
Berkeley), and Andrew Weil (the alternative-medicine guru)
-- the use of both drugs quickly gravitated toward
spiritual, and then frankly recreational uses. At this
point, the drugs themselves were banned, and research ground
to a halt.
Some early "research" on LSD was tragically pointless. A case in point is that of Tusko, an elephant at the Oklahoma City Zoo, who received about 3,000 times the normal human dose of LSD (an attmpted correction for differences in body weight), to see if it would trigger an episode of musth, an episode of aggressive behavior which occurs naturally from time to time in male elephants (West et al., Science, 1962). It didn't. Instead, Tusko suffered a sort of epileptic seizure while his mate, Judy, tried to help him. The whole sad story is told in Elephants on Acid and Other Bizarre Experiments (2007) by Alex Boese. Lesson #2: it's a mistake to think there is a linear relationship between body weight and dose. Lesson #1: don't do stupid, pointless experiments.
Intelligence agencies also took an interest in LSD and other psychedelic drugs. In the 1950s, there was great concern about Soviet and Chinese "brainwashing" of American soldiers and others held captive during the Korean War. The Pentagon and the the CIA experimented with psychedelics, both to develop techniques to resist brainwashing, and to employ in their own mind-control efforts, in a project first known as Project Bluebird and later as MK-ULTRA. MK-ULTRA was first exposed in the 1970s by an investigation headed by Frank Church, a US senator, and by The Search for the Manchurian Candidate (1978) a book by John Marks, an investigative journalist who is the brother of Patricia Marks Greenfield, a psychologist at UCLA. If Leary is the "hero" of LSD research, its antihero is Sidney Gottlieb, a chemist working for the CIA who at one point possessed the entire supply of the drug produced by Sandoz. Gottlieb's story is told in Poisoner in Chief (2019) by the journalist Stephen Kinzer (for a review, see "When the CIA Was Into Mind Control" by Sharon Weinberger, author of Imagineers of War: he Untold Story of DARPA, the Pentagon Agency that Changed the World, an excellent history of the Defense Advanced Research Projects Agency, New York Times, 10/20/2019) MKULTRA never went anywhere, and was discontinued in the 70s -- but not before psychedelics were administered to a large number of unwitting "subjects" -- including Frank Olson, whose LSD-abetted death (he jumped out of a window during a bad trip) is documented in Wormwood (2017), a docudrama mini-series broadcast by Netflix. Lesson #2: don't do stupid, pointless experiments. Documentation of the whole sordid story, including material released by the CIA under the Freedom of Information Act, are available online.
Marks's book took its title from The Manchurian Candidate (1959), a thriller by Richard Condon about an American soldier captured during the Korean War who was brainwashed and sent back to the United States as a sleeper agent. The book was made into a fabulous 1962 movie by John Frankenheimer, and starring Frank Sinatra, Laurence Harvey, Janet Leigh, and Angela Lansbury. The film was remade by Jonathan Demme in 2004; it's good, but try to see the original first. In Condon's book, and the movies, the brainwashing was accomplished through conditioning, not drugs.
 LSD
LSD
 and
the other major psychedelics entered popular culture
in the 1960s, and were prominent features of the
counterculture that emerged in that decade. Much
of the art that papered college dormitory rooms, like
the poster on the left for concerts produced by Bill
Graham in San Francisco, and the
graphics of Peter Max, was dubbed "psychedelic" art.
After participating in one of Ken Keesey's
"acid tests" (popularized by Tom Wolfe in the
Electric Kool-Aid Acid Test. Owsley Stanley,
the audio engineer for the Grateful Dead (image on
right), developed a cottage
industry in his laboratory in
Point Richmond, manufacturing millions of doses
of LSD and other psychedelics for recreational
consumption.
and
the other major psychedelics entered popular culture
in the 1960s, and were prominent features of the
counterculture that emerged in that decade. Much
of the art that papered college dormitory rooms, like
the poster on the left for concerts produced by Bill
Graham in San Francisco, and the
graphics of Peter Max, was dubbed "psychedelic" art.
After participating in one of Ken Keesey's
"acid tests" (popularized by Tom Wolfe in the
Electric Kool-Aid Acid Test. Owsley Stanley,
the audio engineer for the Grateful Dead (image on
right), developed a cottage
industry in his laboratory in
Point Richmond, manufacturing millions of doses
of LSD and other psychedelics for recreational
consumption.
More recently, clinical research on both LSD and psilocybin has restarted, especially targeting anxiety and depression -- including the relief of anxiety and depression in terminally ill patients. And more experimental research has resumed on the effects of these substances on consciousness, and what they can tell us about the neural correlates of consciousness. This revived interest has also led to the development of a new generation of psychedelic drugs, such as nicergoline. There are lots of other ostensibly psychedelic drugs, including some synthetic ones, but these lectures focus on the "classics" of mescaline, psilocybin, and LSD. In contrast with marijuana, where research has focused on its effects on human performance (short-term memory, perceptual-motor coordination, and the like), from the beginning research on the major psychedelics focused on its "consciousness-altering" effects. Presumably, this is because of the religious-spiritual peyote,), literary (mescaline), and countercultural (LSD) context in which these drugs were taken.
In these
lectures, I treat mescaline, psilocybin,
and LSD as one single class of drugs
which have very similar effects on
consciousness.
For a
historical account of the "Cambridge
Quartet" of psychedelic researchers (if
that's
what they were) at Harvard, see The Harvard
Psychedelic Club: How Timothy Leary, Ram
Dass, Huston Smith, and Andrew Weil
Killed the Fifties and Ushered in a New
Age for America by Don Lattin.
See also:
Jackson's Excellent (Alleged) Adventure on Acid
Examiner: "OK, now look at this card, and tell me what you see." Pollack: "Oh, wow!" Examiner: Tell me what you see! Pollack: "Oh, wow!" Examiner: "Jackson, Jackson, tell me what you see!" Pollack: "It's a bat!" |
 Much of
the initial interest in mescaline,
psilocybin, and LSD was
stimulated by these drugs' apparent ability to induce
profound mystical religious, and spiritual
experiences. In an attempt to
capture this aspect of the psychedelic
experiment, Walter Pahnke, a psychiatrist who was also a student
at Harvard Divinity School, conducted what became
known as The Good Friday
Experiment as part of his doctoral
dissertation (supervised by Timothy
Leary, who was at that time on the
psychology faculty at Harvard and
director, with Richard Alpert, of
the Harvard Psilocybin
Project). Pahnke recruited a
number of Protestant divinity
students student from
Andover-Newton Theological Seminary, none of whom had any previous
experience with the drug, and gave
them a dose of psilocybin
during Good Friday services at Boston
University's Marsh Chapel
(got all these institutions straight?). Pahnke
pulled out all the stops: the experiment
was conducted in the basement of Marsh Chapel,
illuminated only by
candlelight, with organ music piped in from the
sanctuary upstairs, along with a
sermon delivered by Howard Thurman, who had been a mentor to Martin Luther King,
Jr. (King had received a doctorate from BU under
Thurman's
guidance). In an attempt
at a double-blind placebo
protocol, half of the subjects received
30 milligrams psilocybin, and
they were matched with subjects who received a
dose of nicotinic acid (vitamin B6),
a central nervous system stimulant, as an
active placebo (the antipsychotic drug
Thorazine was also available for emergencies,
to bring anyone down who experienced
a "bad trip"). However, the
protocol broke down after about 1 hour, when
it became eminently clear who had taken which
substance! An interesting feature of the
Good Friday Experiment was that, at Leary's
insistence, the
research assistants, who were designated
guides, took psilocybin at the same time --
with predictable results. The experiment
became legendary for the chaos that
ensued.
Much of
the initial interest in mescaline,
psilocybin, and LSD was
stimulated by these drugs' apparent ability to induce
profound mystical religious, and spiritual
experiences. In an attempt to
capture this aspect of the psychedelic
experiment, Walter Pahnke, a psychiatrist who was also a student
at Harvard Divinity School, conducted what became
known as The Good Friday
Experiment as part of his doctoral
dissertation (supervised by Timothy
Leary, who was at that time on the
psychology faculty at Harvard and
director, with Richard Alpert, of
the Harvard Psilocybin
Project). Pahnke recruited a
number of Protestant divinity
students student from
Andover-Newton Theological Seminary, none of whom had any previous
experience with the drug, and gave
them a dose of psilocybin
during Good Friday services at Boston
University's Marsh Chapel
(got all these institutions straight?). Pahnke
pulled out all the stops: the experiment
was conducted in the basement of Marsh Chapel,
illuminated only by
candlelight, with organ music piped in from the
sanctuary upstairs, along with a
sermon delivered by Howard Thurman, who had been a mentor to Martin Luther King,
Jr. (King had received a doctorate from BU under
Thurman's
guidance). In an attempt
at a double-blind placebo
protocol, half of the subjects received
30 milligrams psilocybin, and
they were matched with subjects who received a
dose of nicotinic acid (vitamin B6),
a central nervous system stimulant, as an
active placebo (the antipsychotic drug
Thorazine was also available for emergencies,
to bring anyone down who experienced
a "bad trip"). However, the
protocol broke down after about 1 hour, when
it became eminently clear who had taken which
substance! An interesting feature of the
Good Friday Experiment was that, at Leary's
insistence, the
research assistants, who were designated
guides, took psilocybin at the same time --
with predictable results. The experiment
became legendary for the chaos that
ensued.
 But
But 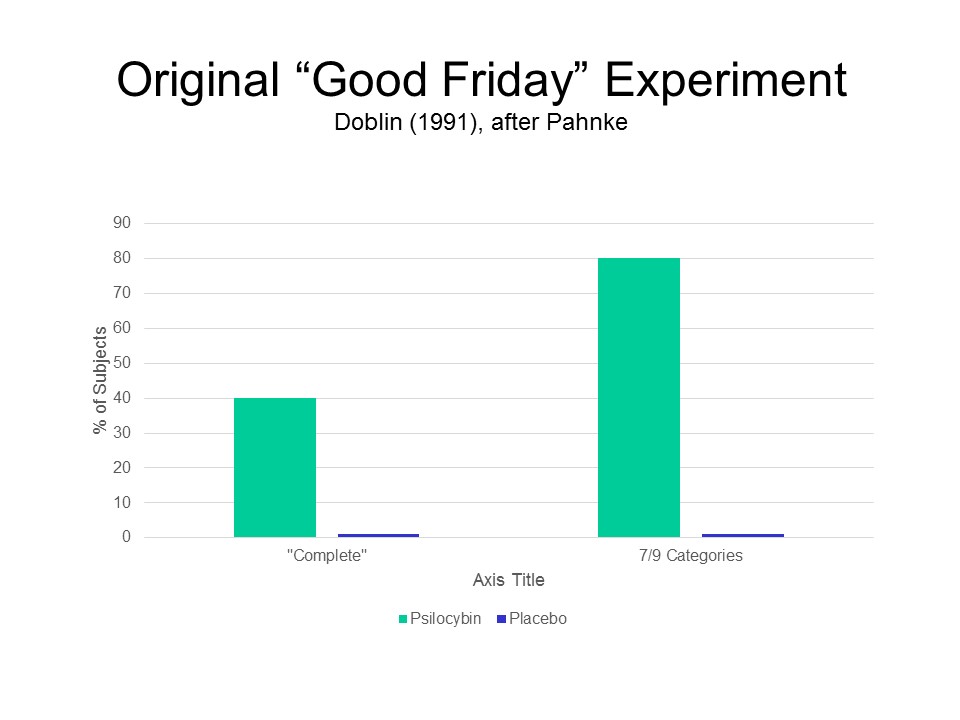 Pahnke tried.
Based on his extensive reading of the
literature on Christian and non-Christian
mystical experiences (he was a divinity
student, after all), he developed a Mystical
Experiences Questionnaire, with a number of
subscales intended to measure changes in the "sense of unity",
transcendence of time and space, sense of
sacredness, and the like. Examples of
the scales of the MEQ are
provided in the table below (numbers refer
to the ordering of items in the full
questionnaire; some questions were filler
items that were not scored). Based on their
responses to the MEQ, Pahnke judged that
40% of the psilocybin group, but none of
the placebo group, had a "complete"
mystical experience. Adopting a
less-stringent criterion, of high scores
on at least 7 of the 9 categories
assessed in the MEQ, 80% of the
psilocybin subjects, but again none of
the placebo subjects, had a mystical
experience during the experiment.
Pahnke tried.
Based on his extensive reading of the
literature on Christian and non-Christian
mystical experiences (he was a divinity
student, after all), he developed a Mystical
Experiences Questionnaire, with a number of
subscales intended to measure changes in the "sense of unity",
transcendence of time and space, sense of
sacredness, and the like. Examples of
the scales of the MEQ are
provided in the table below (numbers refer
to the ordering of items in the full
questionnaire; some questions were filler
items that were not scored). Based on their
responses to the MEQ, Pahnke judged that
40% of the psilocybin group, but none of
the placebo group, had a "complete"
mystical experience. Adopting a
less-stringent criterion, of high scores
on at least 7 of the 9 categories
assessed in the MEQ, 80% of the
psilocybin subjects, but again none of
the placebo subjects, had a mystical
experience during the experiment.
 |
 |
 |
 |
 |
 |
 Pahnke
Pahnke
 also
conducted a followup session with these subjects 6
months after the Good
Friday Experiment., and found that these mystical effects persisted even after
the drugs wore off. It
appeared that a single "trip"
with psilocybin had profound, and long-lasting
effects on the subjects'
personalities. A followup by Doblin
(1991), conducted about 25 years after that
Good Friday, confirmed that the effects were, essentially,
permanent.
also
conducted a followup session with these subjects 6
months after the Good
Friday Experiment., and found that these mystical effects persisted even after
the drugs wore off. It
appeared that a single "trip"
with psilocybin had profound, and long-lasting
effects on the subjects'
personalities. A followup by Doblin
(1991), conducted about 25 years after that
Good Friday, confirmed that the effects were, essentially,
permanent.
In 2025,
a group of researchers
affiliated with Johns
Hopkins University and
New York University
published a sort of
follow-up to the Good
Friday Experiment.
As described by
Michael Pollan, a
journalist who has
sympathetically
chronicled the
resurgence of interest
in psychedelic
experiences, the study
is a textbook example
of how not to
do research ("This is
Your Priest on Drugs",
New Yorker,
05/19/2025). A
miscellaneous group of
clergy and other
religion scholars, all
with no previous
experience with
psychedelics was
recruited through a
magazine ad for a
study of the effects
of psilocybin on
religious
experience. The
sample was small:
roughly 29 subjects
completed the first
session, some of whom
did not return for a
follow-up. There
was no control group
of any kind -- e.g.,
subjects who had no
intrinsic interest in
religion; no placebo
condition, thus no
double-blind (or even
single-blind)
administration of the
drug; even though some
of the subjects were
non-Christians, the
music played during
the session leaned
toward Christian
themes; and some of
the authors of the
study also funded the
study, creating the
potential for
conflicts of
interest.
Although the majority
of subjects reported a
profound religious
experience while on
the drug, some of
which continued to
affect them, it's also
true that at least one
subject was told,
prior to his session,
that he was about to
meet God, raising
questions about what
kinds of expectations
were conveyed to
subjects about their
experience, both
before and during the
procedure. The
study, which as of
this writing was
scheduled to be
published in Psychedelic
Medicine in
2025, isn't worth the
paper it's printed
on. But Pollan's
article is very well
worth reading, for its
sensitive discussion
of the links between
psychedelic drugs and
religion.
 A
A  somewhat more secular
approach was taken by Harriet Linton-Barr,
Robert Langs, and
their colleagues at the Postgraduate
Center for Mental Health, a
psychoanalytically oriented research
group affiliated
with New York University (Linton
and Langs, 191962a, 1962b, 1964;
Linton et al., 1964; Langs, 1967,
1971; Langs & Barr, 1968; all
of this research is summarized in
Linton Barr, Langs,
et al., 1972).
Their subjects, who
were naive to LSD
(which almost everyone was in
1959), and judged to be in good
mental health, received 100
micrograms of LSD; controls
received a placebo of lemon
juice in water.
That's
not a very good placebo, of
course, not even as good as
the nicotinic acid used in
Pahnke's
Good Friday Experiment.
But really, when it comes to
LSD and psilocybin, it's
pretty clear that subjects
can tell pretty quickly then they've
gotten the placebo, so it's
probably just as
well not to be a stickler about
it. Anyway, the subjects
completed a number of
tests both
before and after ingesting the
drug,
including:
somewhat more secular
approach was taken by Harriet Linton-Barr,
Robert Langs, and
their colleagues at the Postgraduate
Center for Mental Health, a
psychoanalytically oriented research
group affiliated
with New York University (Linton
and Langs, 191962a, 1962b, 1964;
Linton et al., 1964; Langs, 1967,
1971; Langs & Barr, 1968; all
of this research is summarized in
Linton Barr, Langs,
et al., 1972).
Their subjects, who
were naive to LSD
(which almost everyone was in
1959), and judged to be in good
mental health, received 100
micrograms of LSD; controls
received a placebo of lemon
juice in water.
That's
not a very good placebo, of
course, not even as good as
the nicotinic acid used in
Pahnke's
Good Friday Experiment.
But really, when it comes to
LSD and psilocybin, it's
pretty clear that subjects
can tell pretty quickly then they've
gotten the placebo, so it's
probably just as
well not to be a stickler about
it. Anyway, the subjects
completed a number of
tests both
before and after ingesting the
drug,
including:
 Repeated
Repeated  measures on the
total questionnaire score showed that LSD had its peak effect
about 2-5 hours after administration, and had worn off by the
time of final testing the next day.
The Stroop test showed a substantial interference effect while
on the drug, but this was no different from that observed in
the placebo group. However, we now know Stroop
interference is a good index -- some call
it the "gold standard" of automaticity. Linton and
Langs didn't
know about automaticity, however, it in the future it would
be interesting to compare the effects of LSD on both
automatic and controlled processes.
measures on the
total questionnaire score showed that LSD had its peak effect
about 2-5 hours after administration, and had worn off by the
time of final testing the next day.
The Stroop test showed a substantial interference effect while
on the drug, but this was no different from that observed in
the placebo group. However, we now know Stroop
interference is a good index -- some call
it the "gold standard" of automaticity. Linton and
Langs didn't
know about automaticity, however, it in the future it would
be interesting to compare the effects of LSD on both
automatic and controlled processes.
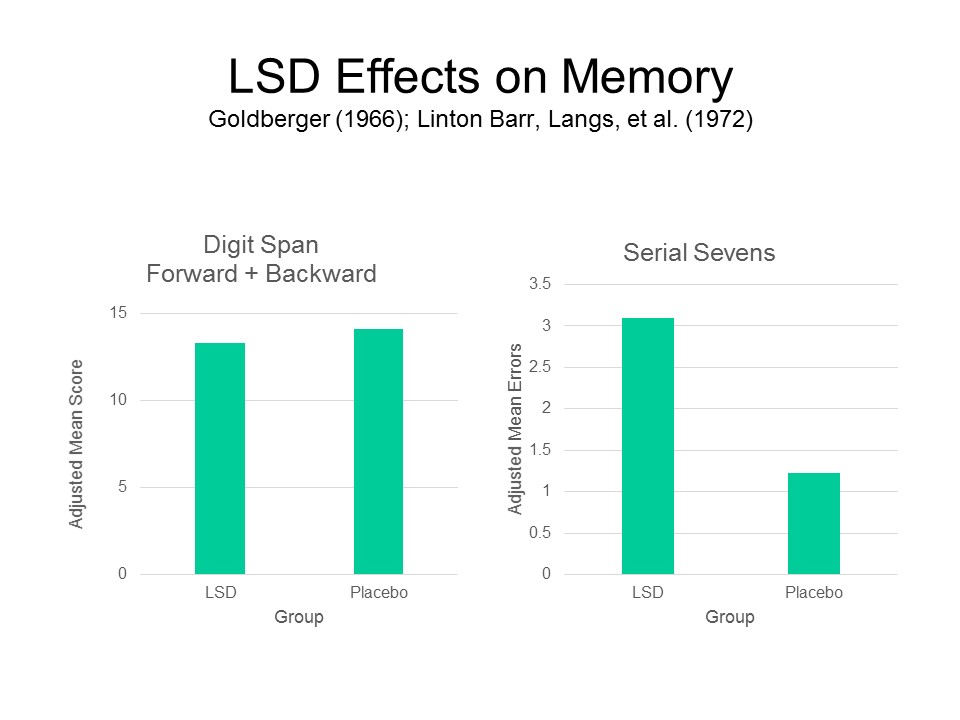 And given Pollan's remarks
about short-term memory and the mystical
experience under marijuana, a good test of memory functions
would be in order as well. Linton
Bar, Langs, et al. found no effect of
LSD on Digit Span performance, but did find
profound effects on the more cognitively
demanding Serial Sevens
task.
And given Pollan's remarks
about short-term memory and the mystical
experience under marijuana, a good test of memory functions
would be in order as well. Linton
Bar, Langs, et al. found no effect of
LSD on Digit Span performance, but did find
profound effects on the more cognitively
demanding Serial Sevens
task.
As  part of the effort to revive the
therapeutic uses of psychedelic drugs
(see below), Roland Griffiths
et al. (2006), with
the Psilocybin Research Initiative at Johns
Hopkins University Medical School,
conducted a replication of Pahnke's
Good Friday Experiment with
additional controls. They recruited by
advertising for adults with a
history of "religious" or
"spiritual" participation, who
had no prior experience with
psilocybin or other
hallucinogens. The
experiment was conducted in a medical
laboratory, not a chapel (and not on Good
Friday, either!);
the subjects wore
masks to block
extraneous stimuli,
and listened to
classical
music.
Following a
double-blind
protocol, some
subjects received 30
milligrams
of psilocybin;
controls received a
dose of
methylphenidate,
better known as
Ritalin, a more CNS
stimulant
than nicotinic
acid (and thus,
arguably, a better
active
placebo).
Assessing mystical
experiments with a
variant on Pahnke's
MEQ,
known as the
Pahnke-Richards
Mystical
Experiences
Questionnaire,
they found elevated
scores on all
scales,
compared to
the placebo
group.
In a follow-up
study, additionally
employing
a
new Persisting
Effects
Questionnaire,
study,
the
scores of the
psilocybin
group continued
to be elevated
-- in fact,
hardly
unchanged! --
14
months
later,
with no
untoward
effects.
Griffiths et
al. concluded,
as stated in
the title of
their paper,
that a single
dose of
"[p]silocybin
can occasion
mystical-type
experiences
having
substantial
and sustained
personal
meaning and
spiritual
significance".
In their view,
effects like
these justify
clinical
trials on the
use of
psilocybin
to relieve
anxiety and
depression in
cancer
patients.
part of the effort to revive the
therapeutic uses of psychedelic drugs
(see below), Roland Griffiths
et al. (2006), with
the Psilocybin Research Initiative at Johns
Hopkins University Medical School,
conducted a replication of Pahnke's
Good Friday Experiment with
additional controls. They recruited by
advertising for adults with a
history of "religious" or
"spiritual" participation, who
had no prior experience with
psilocybin or other
hallucinogens. The
experiment was conducted in a medical
laboratory, not a chapel (and not on Good
Friday, either!);
the subjects wore
masks to block
extraneous stimuli,
and listened to
classical
music.
Following a
double-blind
protocol, some
subjects received 30
milligrams
of psilocybin;
controls received a
dose of
methylphenidate,
better known as
Ritalin, a more CNS
stimulant
than nicotinic
acid (and thus,
arguably, a better
active
placebo).
Assessing mystical
experiments with a
variant on Pahnke's
MEQ,
known as the
Pahnke-Richards
Mystical
Experiences
Questionnaire,
they found elevated
scores on all
scales,
compared to
the placebo
group.
In a follow-up
study, additionally
employing
a
new Persisting
Effects
Questionnaire,
study,
the
scores of the
psilocybin
group continued
to be elevated
-- in fact,
hardly
unchanged! --
14
months
later,
with no
untoward
effects.
Griffiths et
al. concluded,
as stated in
the title of
their paper,
that a single
dose of
"[p]silocybin
can occasion
mystical-type
experiences
having
substantial
and sustained
personal
meaning and
spiritual
significance".
In their view,
effects like
these justify
clinical
trials on the
use of
psilocybin
to relieve
anxiety and
depression in
cancer
patients.
In 2019, Hopkins obtained $17 million in private
donations and investments (!) to establish a Center for
Psychedelic and Consciousness Research, with Griffiths as its
director, with the goal of studying the efficacy of LSD,
psilocybin, and other psychedelics in the treatment of various
forms of mental illness, coping with medical problems such as
AIDS, and end-of-life care. A similar center, also
privately funded, has been established at Imperial College
London. See "Johns Hopkins Opens New Center for Psychdelic
Research", and "Tim Ferriss, the Man Who Put His oney Behind
Psychedelic Medicine" both by Benedict Carey, New York Times,
09/10/2019).
The Ecstasy and the Agony of Julian of NorwichAt age thirty, Julian experienced sixteen extended and agonizing visions of God, which she collected in a book called "Revelations of Divine Love". She describes feeling "a supreme spiritual pleasure in my soul" and being "filled with eternal certainty," a feeling "so joyful in me and so full of goodness that I felt completely peaceful, easy and at rest, as though there were nothing on earth that could hurt me". But, she writes, "this only lasted for a while, and then my feeling was reversed and I was left oppressed, weary of myself, and so disgusted with my life that I could hardly bear to live"Well, maybe Ecstasy is the path to God and maybe not. But what strikes me as more interesting is the aftermath of Julian's experiences. She didn't just come back down to earth, as it were. Instead, her emotional state went below zero, to something like its hedonic opposite: joy was replaced by disgust. This is exactly what we would predict from what is known as the opponent-process theory of acquired motivation, which I discuss at length in my introductory course. Briefly, the opponent-process theory postulates that every affective state (call if the "A State") invokes its hedonic opposite (call it the "B State") as a sort of slave state. When the stimulus that elicited the A State disappears, the B state comes rushing in with a vengeance. These temporal dynamics of affect predict the "high", tolerance, and withdrawal associated with drug addiction -- and further suggest that addiction itself is motivated more by the desire to avoid the agonies of withdrawal than by the desire to obtain the pleasures of the high. Be that as it may, one wonders if the opponent-process theory applies to mystical experiences as well: if they are followed by crashes rather than a simple return to baseline; and whether something like tolerance occurs as a result of their repetition. |
Aside from its recreational uses, LSD came to
the attention of researchers because of its potential use in
psychotherapy, especially for alcoholism and drug abuse.
These clinical uses spurred experimental research on their
psychological and physiological effects. However,
experimental research and clinical practice was soon
contaminated by recreational use (think timothy Leary). As a
result, the US Food and Drug Administration (FDA) classified
all hallucinogenic drugs as "Schedule I" drugs, with no
medical use, and essentially shutting down basic research as
well. However, psychotherapeutic interest in psychedelics
has recently been revived, and it is now possible to read
reports in professional journals of preliminary clinical
studies of the effectiveness of LSD, psilocybin, and even
ketamine "(Special K", a powerful anesthetic) and MDMA
(Ecstasy, better known at "the date-rape drug") in the
treatment of post-traumatic stress disorder (PTSD), anxiety
and depression (including anxiety and depression secondary
to cancer), and alcohol and drug
abuse (see 'Hallucinogens as Medicine" by Roland Griffiths
and Charles Grob, Scientific American, 12/2010; "The Trip Treatment" by Michael Pollan, New
Yorker, 02/09/2015; "High Science" by Hampton Sides,
National Geographic, 06/2015). Like
marijuana, the major psychedelics have also been used in the
treatment of anxiety and depression associated with medical
illnesses, such as cancer. Most of this research has
focused on marijuana (which is gradually being legalized, at
least at the state level) and psilocybin (which is a natural as opposed to synthetic
compound, with a long history of use by indigenous people
in the Americas, and doesn't have the "outlaw" and
"countercultural" connotations of LSD).
In 2021, the first
randomized controlled "Phase 3" trial of MDMA was
published, with promising results (Mitchell et al., Nature
Medicine, 2021). A heterogeneous group of
patients with a diagnosis of post-traumatic stress
disorder (PTSD) was administered a low dose of MDMA under
controlled, supervised conditions, along with talk
therapy; a control group received a placebo instead of the
active drug. The patients immediately knew which
group they were in, which can't be helped in these sorts
of studies, so the study design was not "double-blind",
but at least the clinicians evaluating the outcome of
treatment were blind). Two months after treatment
was completed, 67% of the patients in the drug group, but
only 32% of those in the placebo group, showed symptom
remission such that they no longer qualified for a
diagnosis of PTSD. None of the patients in the drug
group showed any serious side effects.
Interestingly, the MDMA does not act on its own, and must
be used as an adjunct to psychotherapy in order to be
effective (the three MDMA sessions were spaced about a
month apart, while the patients were receiving
psychotherapy). In this case, But unlike other
psychotropic drugs, it seems to do more than dampen
symptoms (the way, for example, antipsychotic drugs act on
schizophrenia). The study was supported by the
Multidisciplinary Association for Psychedelic Studies, a
nonprofit research group directed by Rick Doblin -- who,
as noted earlier, led the replication of the "Good Friday
Experiment". Before MDMA can hope to be approved for
therapeutic use by the Food and Drug Administration, there
has to be a second positive Phase 3 trial, which is
currently underway. If these results are confirmed,
the door may be opened to formal studies, and perhaps FDA
approval, for other psychedelics, such as LSD.
Don't try this at home! MDMA purchased on the street is likely to be far more potent than the doses used in this study, and may be adulterated with various toxic substances. If you suffer from PTSD, get your family physician to refer you to a qualified mental-health practitioner for treatment.
If the initially positive results hold up, the
clinical success may lay the foundation for more
experimental research on the psychological effects of
psychedelic drugs. At present, however, potential
investigators are bound by the same legal constraints as
affected potential investigators generations ago. In the
current instance, for example, the fact that psychedelic
drugs are illegal has forced investigators to get funding
from a private foundations, chiefly the the
Multidisciplinary Association for Psychedelic Studies (MAPS;
founded by Rick Doblin, who led the replication of the "Good
Friday Experiment), and the Heffter Research Institute. MAPS
and the Hefter Institution also sponsor an annual
"Psychedelic Science" conference: the 2012 and 2013 meetings
were held, of course, in Oakland, home of Oaksterdam
University. The hope is that the success of these small,
privately funded clinical trials will spur interest on the
part of government agencies, such as the Defense Department
(for treatment of PTSD in veterans), NIMH (anxiety
disorders, depression), NIDA and NIAAA (for substance
abuse), and NIH (for cancer and other life-threatening
illnesses). Meanwhile, in California and other states,
taxes on medical and recreational marijuana are being used
to subsidize new research on medical applications of both
major and minor psychedelics.
Unfortunately, in many of these small, privately funded clinical studies, there are none of the usual controls to determine the actual source of any effects. The patients typically receive the drug in the context of ongoing psychotherapy, so we do not know whether the effects are due to the drug the psychotherapy, or some combination; there is no random assignment, so we don't know about selection effects. . The trials are not run double-blind (or even single-blind), and there is no control for patient (or investigator) expectations that might give rise to placebo effects. And, as with medical marijuana today, there is always the danger that recreational use will be confused with clinical and research use, threatening the entire research enterprise, and fostering ignorance of the effects of these substances and their theoretical implications.
Unfortunately, research
on marijuana has been stymied by the fact that, even though
sales of the substance are legal in states like Colorado
(and, to a lesser extent, California and Oregon), as
of 2015, scientific and medical researchers must
procure their marijuana from a single government-approved
supplier (affiliated with the University of Mississippi, no
less!). The problem is that this "official" crop of
marijuana contains much less tetrahydrocannabinol (THC) and
cannabidiol (CBD), the primary ingredients in marijuana,
than what is currently being sold for medical use and
personal consumption (THC gives users their euphoric "high",
but some research indicates that CBD has therapeutic effects
in the treatment of post-traumatic stress disorder).
Therefore, the findings of officially sanctioned marijuana
research may not generalize outside the laboratory, where
"high-grade" marijuana is actually in use.
The situation with respect
to other psychedelic substances is even worse, as there
are no licensed suppliers for drugs such as LSD
and psilocybin.
Still, the increasing
interest in the psychotherapeutic uses of pychedelic drugs
has led to a revival of purely experimental research on
drug-induced alterations in consciousness. In the
first modern study of this type, a group of British
investigators employed a double-blind, placebo-controlled
study to show that microdoses (5-20 micrograms) of LSD
significantly distorted time-perception (Yanakieva et al.,
Psychopharmacology, 2019).
Not
to be outdone,
in 2020 UCB
established
the UC
Berkeley
Center for the
Science of
Psychedelics
to support
research and
pubic
education.
Founded with a
grant from an
anonymous
donor, the
center will
support basic
research on
the effects of
psychedelic
substances,
especially
psilocybin and
"psychedelic
plants", on
perception,
cognition, and
emotion and
their
biological
substrates.
This basic
research,
conducted with
healthy
subjects, is
intended to
complement the
clinical
research going
on at Hopkins,
Imperial
College
London, and
elsewhere.
Drawing on the
resources of
the Graduate
Theological
Union, it will
also study the
relation
between
psychedelic
experiences
and
spirituality.
See, for
example, "A
Psychedelic
for Trauma" by
Jennifer M.
Mitchell, a
psychiatrist
at UCSF and
member of the
Berkeley
Center, Scientific
American,
02/2022.
For an account of this revival, see Neuropsychedelia: The Revival of Hallucinogen Research Since the Decade of the Brain (2012), by Nicholas Langlitz, an anthropologist.
Also How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, and Transcendence (2018) by Michael Pollan, who wrote so enthusiastically about psychedelics in his 2001 book, The Botany of Desire. See also This is Your Mind on Plants (2021), which goes into some detail on three mind-altering plants: opium (which Pollan himself actively cultivated), caffeine (!), and mescaline (reviewed by Kiki Sanford in "Medicinal Plants, in Context", Science, 07/09/2021; and by Mike Jay in "The Well-Blown Mind", New York Review of Books, 09/23/2021). Pollan points out that current research on psychedelics continues to suffer from the "countercultural baggage" of the 1960s (Timothy Leary and all that), which led to a kind of moral panic, which led to the almost-total curtailment of scientific research on psychedelics and their effects. Pollan suggests that the true value of psychedelics lies not in the immediate experience of psychedelic intoxication -- what John Williams, reviewing Pollan's book in the New York Times, calls "the grooviness of the moment", but rather in the insights about self, social relationships, and other deeply personal matters that remain in memory after the drugs have worn off ("A Straight-Laced Writer Explores Psychedelics, and Leaves the Door of Perception Ajar", 05/15/2018). Research on therapeutic applications of psychedelics, if it yields positive results, could normalize psychedelic drugs, much as yoga and meditation are normalized today.
For an account of the earliest days of the Psychedelic Revolution -- the days before Leary and Alpert and the War on Drugs, see Tripping on Utopia: Margaret Mead, the Cold War, and the Troubled Birth of Psychedelic Science by Benjamin Breen (2024), reviewed by Margaret Talbot in "Acid Reflux", New Yorker, 01/29/2024, from which the following quotes are drawn). Talbot writes that "The psychedelic flowering of the sixties has, it turns out, a prequel -- a rich and partly forgotten chapter before the hippie movement, before the shamanistic preening and posturing of Timothy Leary, and before the war on drugs shut all that down." Major figures in that prequel were the anthropologists Margaret Mead and her husband, Gregory Bateson, who served as "spiritual guides", "owing to their shared vision of science as a tool for expanding consciousness -- so that, in Mead's words, we "reach an awareness which will give us a new control over our human destiny" and "learn consciously to create a civilization within which an increasing proportion of human beings will realize more of what they have it in them to be". Injecting a cautionary note, Bateson "lamented that people were seeking 'short cuts to wisdom' through LSD". Despite all the attention given to the new "psychedelic medicine", Breen believes that psychedelic drugs will never attain the vaunted status of prescription medicines, because they are put to so many varied uses. For this reason, they may properly belong to an entirely new category of substances.
For a timely review of psychedelic therapy, see "Therapeutic Potential of Psychedelic Drugs: Navigating High Hopes, Strong Claims, Weak Evidence, and Big Money" by K. Humphreys, P.T. Korthuis, D. Stjepanovic, and W. Hall, Annual Review of Psychology, 2025.
This page last modified 05/22/2025.