Further Reading on HypnosisLink to a general introduction to hypnosis, adapted from Kihlstrom, J.F. (1998). Hypnosis and the psychological unconscious. In H.J. Friedman (Ed.), Encyclopedia of mental health (Vol. 2, pp. 467-477). San Diego: Academic Press. Link to another general introduction, by Michael Nash, reprinted from Scientific American (July 2001). Link to a fuller discussion of the same issues, reprinted from Kihlstrom, J.F. (2008). The domain of hypnosis, revisited. In M. Nash & A. Barnier (Eds.), Oxford handbook of hypnosis (pp. 21-52). Oxford: Oxford University Press. Link to a discussion of consciousness in hypnosis, reprinted from Kihlstrom, J.F. (2007). Consciousness in hypnosis. In P.D. Zelazo, M. Moscovitch, & E. Thompson (Eds.), Cambridge handbook of consciousness (pp. 445-479). Cambridge: Cambridge University Press. Link to a discussion of hypnosis and pain control: Kihlstrom, J.F. (2000, November). Hypnosis and pain: Time for a new look. Plenary address presented at the annual meeting of the American Pain Society, Atlanta. Link to a further discussion of hypnosis and pain control: Kihlstrom, J.F. (2001, August). Hypnosis in surgery: Efficacy, specificity, and utility. Paper presented at the annual meeting of the American Psychological Association, San Francisco. |
 Hypnosis is a social
interaction in which one participant, designated the subject,
responds to suggestions offered by another participant,
designated the experimenter, for imaginative experiences
involving alterations in perception, memory, and the voluntary
control of action. In the classic case, response to these
suggestions is accompanied by subjective conviction bordering
on delusion and the experience of involuntariness bordering on
compulsion.(The image shows Prof. David
Spiegel, a psychiatrist at Stanford University, working with
a hypnotic subject.)
Hypnosis is a social
interaction in which one participant, designated the subject,
responds to suggestions offered by another participant,
designated the experimenter, for imaginative experiences
involving alterations in perception, memory, and the voluntary
control of action. In the classic case, response to these
suggestions is accompanied by subjective conviction bordering
on delusion and the experience of involuntariness bordering on
compulsion.(The image shows Prof. David
Spiegel, a psychiatrist at Stanford University, working with
a hypnotic subject.)
Since the end of the 19th century hypnosis has
been considered to be a laboratory model for the "hysterical"
(i.e., dissociative and conversion) disorders sometimes seen
in the clinic. That is, many of the cognitive and emotional
changes produced by hypnotic suggestion are similar to those
seen in the dissociative and conversion disorders. For
example, psychogenic amnesia, fugue, and the interpersonality
amnesia of multiple personality disorder have parallels to
posthypnotic amnesia. Hypnotically induced blindness,
deafness, and paralysis are phenotypically similar to
"hysterical" blindness, deafness, and paralysis.
T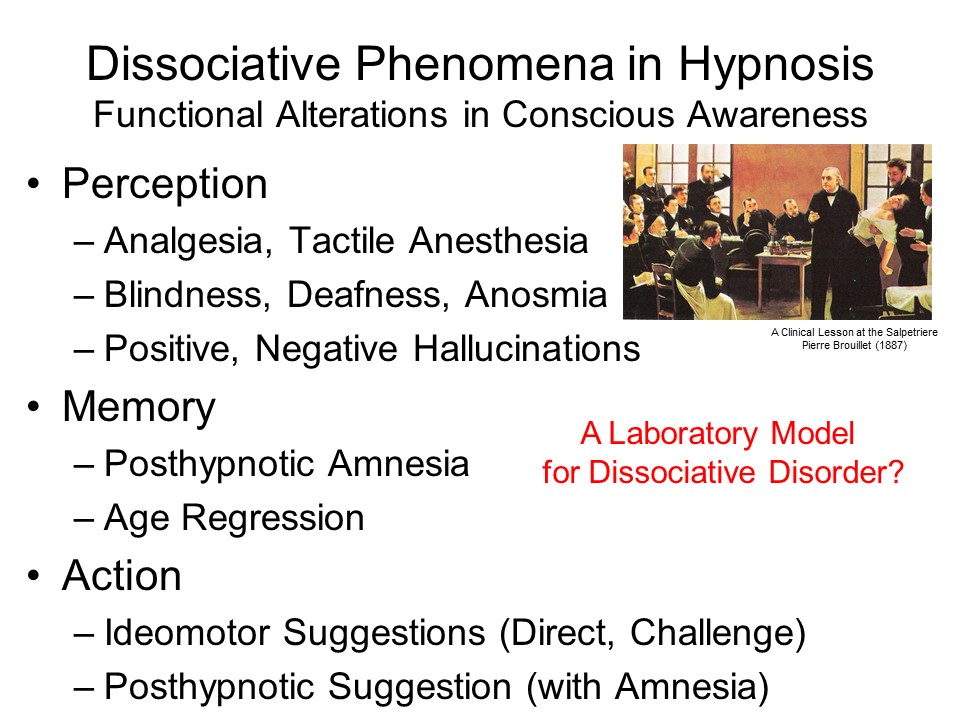 his image shows a painting, "A Clinical Lesson
at the Salpetriere", by Pierre Brouillet, 1887, depicting
Charcot demonstrating hypnosis.
Charcot, in whose clinic Sigmund Freud
studied both hysteria and hypnosis,
believed that hysterical patients were highly
hypnotizable, and that highly hypnotizable people were
prone to hysteria. We now know that there is no
correlation between hypnotizability
and mental illness -- except,
perhaps, that people who are well-adjusted are
more responsive to hypnosis than those who are
disturbed.w
his image shows a painting, "A Clinical Lesson
at the Salpetriere", by Pierre Brouillet, 1887, depicting
Charcot demonstrating hypnosis.
Charcot, in whose clinic Sigmund Freud
studied both hysteria and hypnosis,
believed that hysterical patients were highly
hypnotizable, and that highly hypnotizable people were
prone to hysteria. We now know that there is no
correlation between hypnotizability
and mental illness -- except,
perhaps, that people who are well-adjusted are
more responsive to hypnosis than those who are
disturbed.w
The origins of hypnosis extend to the ancient temples of Aesculapius, the Greek god of medicine, where the advice and reassurance uttered by priests to patients while they slept was interpreted by the patients as the gods speaking to them in their dreams,
The more recent history of hypnosis begins with Franz Anton Mesmer, an 18th-century Austrian physician who believed that disease in various organs was caused by an imbalance of animal magnetism -- an imbalance which could be corrected by a crisis elicited when the "magnetizer" passed his hands over the patient.
Mesmer's theories were discredited by a French royal
commission, but his practices persisted. When the Marquis de
Puysegur experimented with animal magnetism, Victor Race, a
peasant on his estate, fell into a sleep-like state instead of
a magnetic crisis. During this state, Victor was highly
responsive to instructions, and awoke with an amnesia for what
had occurred during the sleep. This incident is the beginnings
of hypnosis as we know it today.
For an excellent survey of the Royal Commissions to Investigate Animal Magnetism (there were too), see the excellent, thoroughly documented, and defintive Wikipedia article by Lindsay Yeates, an Australian psychotherapist who is also a trained historian.
In the mid 19th century, mesmerism was picked up by the British physicians Elliotson and Esdaile. Braid coined the term hypnotism, and speculated that the state was due to the subject's concentration on a single thought. In the late 19th century, hypnosis was studied in France by Charcot, Janet, Bernheim, and Freud. Charcot thought that hypnosis was a form of hysteria, and Freud's observation of hysterics' response to hypnotic suggestions was the origin of his psychogenic theory of mental illness.
The French revival of hypnosis was carried to America by William James and Morton Prince. P.C. Young and C.L. Hull began a tradition of experimental work which declined during the heyday of behaviorism, and was revived in the 1950s by T.R. Sarbin, E.R. Hilgard, J. P. Sutcliffe, M.T. Orne, and T.X. Barber. Their students (Orne was my mentor in graduate school), and their students' students in turn, created an upsurge of experimental work beginning in the 1960s and 1970s that continues to this day.
 In one way or
another, research on hypnosis has been
framed by a debate between what Sutcliffe
(1960, 1961) called the "credulous" and the "skeptical"
views of hypnotic phenomena.
In one way or
another, research on hypnosis has been
framed by a debate between what Sutcliffe
(1960, 1961) called the "credulous" and the "skeptical"
views of hypnotic phenomena.
Let us note, in passing, that nobody ever doubted that H.M. was amnesic, or that Weiskrantz's blindsight patient, R.N., was blind -- because they had brain damage. Which leads me, in my more cynical moments, to reflect on what I have called the irony of self-reports -- which is that all too many psychologists take self-reports seriously only when they are made by people who are brain-damaged!. But I digress.
 Similarly, E.R. Hilgard
offered a neodissociation view, that hypnosis entails a
division in consciousness. That is, the subject is unaware
of certain percepts, memories, thoughts, etc. that nevertheless
continue to influence his behavior unconsciously -- that is,
outside of conscious awareness and conscious control.
Similarly, E.R. Hilgard
offered a neodissociation view, that hypnosis entails a
division in consciousness. That is, the subject is unaware
of certain percepts, memories, thoughts, etc. that nevertheless
continue to influence his behavior unconsciously -- that is,
outside of conscious awareness and conscious control. We'll return to these and other theoretical points of view
later. For now, let's focus on empirical research on the
various phenomena of hypnosis/
The most important single fact about hypnosis is the existence of individual differences in response to suggestion. However, hypnotizability cannot be predicted by the usual sort of psychological tests. Instead, it must be measured by work samples of hypnotic response, analogous to the performance tests used for measuring intelligence.
 Of these
standardized scales, the best known are the Stanford Hypnotic
Susceptibility Scales and the Harvard Group Scale of Hypnotic
Susceptibility. Alternative scales have been published,
but the Stanford Hypnotic Susceptibility Scale, Form C is
generally considered to be the "gold standard" for measuring
hypnotizability. In typical practice, the Harvard Scale
is administered first, to acquaint subjects with hypnosis,
followed by the Stanford Form C.
Of these
standardized scales, the best known are the Stanford Hypnotic
Susceptibility Scales and the Harvard Group Scale of Hypnotic
Susceptibility. Alternative scales have been published,
but the Stanford Hypnotic Susceptibility Scale, Form C is
generally considered to be the "gold standard" for measuring
hypnotizability. In typical practice, the Harvard Scale
is administered first, to acquaint subjects with hypnosis,
followed by the Stanford Form C.
 The
The  hypnotizability scales, administered to
unselected samples, yield a roughly normal distribution of
scores, with a plurality of subjects scoring as relatively
insusceptible to hypnosis, and only
about 10-15% of the population classifying as hypnotic
"virtuosos". It is in these highly responsive individuals that
hypnosis is most appropriately studied. There's no point in
studying hypnosis in subjects who are incapable of
experiencing it.
hypnotizability scales, administered to
unselected samples, yield a roughly normal distribution of
scores, with a plurality of subjects scoring as relatively
insusceptible to hypnosis, and only
about 10-15% of the population classifying as hypnotic
"virtuosos". It is in these highly responsive individuals that
hypnosis is most appropriately studied. There's no point in
studying hypnosis in subjects who are incapable of
experiencing it.
Perhaps the most dramatic perceptual-cognitive alterations associated with hypnosis is hypnotic analgesia, which lies somewhere in between the content-specific negative hallucinations and the modality-specific anesthesias. Beginning with the work of Esdaile and Elliotson, British physicians serving in colonial India in the 1840s, before the introduction of ether and other chemical anesthetics and analgesics, hypnosis has served as the sole anesthetic for a wide variety of surgical procedures, including appendectomy, skin grafts, cardiac surgery, orthopedic surgery, the ligation and stripping of varicose veins, and, especially, obstetrics, including vaginal deliveries and caesarian sections.
|
Link to a discussion of hypnosis and pain control: Kihlstrom, J.F. (2000, November). Hypnosis and pain: Time for a new look. Plenary address presented at the annual meeting of the American Pain Society, Atlanta. Link to a further discussion of hypnosis and pain control: Kihlstrom, J.F. (2001, August). Hypnosis in surgery: Efficacy, specificity, and utility. Paper presented at the annual meeting of the American Psychological Association, San Francisco. |
Esdaile's and Elliotson's early clinical reports excited much interest - -although after Morton's successful demonstration of ether analgesia in 1847, hypnosis was quickly supplanted by ether and other chemical anesthetics. Against the skepticism of his colleagues, Esdaile simply pointed to the fact that his patients eagerly referred their friends and family members to him for treatment.
 |
 |
 Clinical reports
published since the mid-19th century indicate that hypnotic
analgesia can be highly effective in relieving the pain of
major surgery (for reviews of this literature, see Hypnosis
in the Relief of Pain by E.R. Hilgard and J.R. Hilgard,
1975). However, the more common clinical use of analgesia is
in the treatment of postoperative pain, episodic pain
associated with specific medical and surgical procedures;
burns; obstetrics; dentistry; and chronic pain associated with
illness. There is also an extensive body
of experimental laboratory research, making hypnotic
analgesia the most thoroughly studied of all the phenomena
of hypnosis.
Clinical reports
published since the mid-19th century indicate that hypnotic
analgesia can be highly effective in relieving the pain of
major surgery (for reviews of this literature, see Hypnosis
in the Relief of Pain by E.R. Hilgard and J.R. Hilgard,
1975). However, the more common clinical use of analgesia is
in the treatment of postoperative pain, episodic pain
associated with specific medical and surgical procedures;
burns; obstetrics; dentistry; and chronic pain associated with
illness. There is also an extensive body
of experimental laboratory research, making hypnotic
analgesia the most thoroughly studied of all the phenomena
of hypnosis.
 More
More  recent controlled clinical trials confirm
what Esdaile and Elliotson knew: hypnotic suggestions for
analgesia. Viewed in terms of effect size, the
power of hypnotic suggestions corresponds to a "strong" effect,
averaging d >.60, in both clinical and experimental
situations. These effects are especially strong in
patients and subjects who are relatively high in
hypnotizability.
recent controlled clinical trials confirm
what Esdaile and Elliotson knew: hypnotic suggestions for
analgesia. Viewed in terms of effect size, the
power of hypnotic suggestions corresponds to a "strong" effect,
averaging d >.60, in both clinical and experimental
situations. These effects are especially strong in
patients and subjects who are relatively high in
hypnotizability.
 Among the most interesting recent clinical
studies was by Lang et a. (2000), who employed hypnotic
analgesia as an adjunct to conscious sedation in outpatient
diagnostic surgery (for example, arthroscopic examination of the
knee; a common PCA device is
illustrated on the left). All these patients received
patient-controlled conscious sedation, in which they were able
to self-administer (within limits) benzodiazepine-like drugs
that induce sedation and pain relief without loss of
consciousness (for more information, see the lectures on "Anesthesia
and Coma"; see also the section on Conscious Sedation in
the lectures on "Psychedelics").
These
patients were then randomly assigned to receive one of two
adjunctive behavioral treatments -- that is, treatments
delivered in addition to the sedative drug: either
hypnotic suggestions for relaxation, reveries, and analgesia; or
a nonhypnotic attentional manipulation intended to distract the
patient from the procedure and its consequent pain).
Among the most interesting recent clinical
studies was by Lang et a. (2000), who employed hypnotic
analgesia as an adjunct to conscious sedation in outpatient
diagnostic surgery (for example, arthroscopic examination of the
knee; a common PCA device is
illustrated on the left). All these patients received
patient-controlled conscious sedation, in which they were able
to self-administer (within limits) benzodiazepine-like drugs
that induce sedation and pain relief without loss of
consciousness (for more information, see the lectures on "Anesthesia
and Coma"; see also the section on Conscious Sedation in
the lectures on "Psychedelics").
These
patients were then randomly assigned to receive one of two
adjunctive behavioral treatments -- that is, treatments
delivered in addition to the sedative drug: either
hypnotic suggestions for relaxation, reveries, and analgesia; or
a nonhypnotic attentional manipulation intended to distract the
patient from the procedure and its consequent pain).
| Patients receiving hypnosis plus PCA reported much less pain than those receiving either PCA alone or PCA plus the attention manipulation -- especially during the latter stages of the surgical procedure. |  |
| They also reported much less anxiety during the surgical procedure. |  |
| And they made fewer requests for additional medication -- perhaps the ultimate behavioral proof that they actually felt less pain. (Because of external safety controls, not all requests for PCA result in the actual delivery of medication.) Note that the hypnosis and attention groups were equivalent in that regard. However, there is other evidence, reviewed below, suggesting that hypnosis is not simply a form of distraction. |  |
| Finally,
there were fewer adverse events during surgery when
hypnosis was added to the PCA ("adverse event" doesn't
necessarily mean something big,
like the surgeon losing a sponge or a scalpel.
Rather, in surgery, "adverse event" refers to any
occasion where the surgery had to be
interrupted. On a practical level, this means
that the addition of hypnosis, despite the extra
expense of the hypnotist (if the anesthesiologist
himself doesn't perform this task),
is actually more cost-effective. In fact, a later report by Lang & Rosen (2002) indicated that adding hypnosis to PCA actually reduced the average cost of anesthesia by more than 50%. |
 |
Actually, Lang's study has a precedent, dating from the earliest years of surgical anesthesia. Quoting from an internet listserv posting by Dr. Dabney Ewin:
At a time when anesthetic deaths at University Hospitals were reported at one in four hundred anesthetics, Alice Magaw reported 14,380 consecutive cases without a death. Her father was a lay hypnotist who had taught her hypnosis. She wrote:
"Suggestion is a great aid in producing a comfortable narcosis ... during the administration, the anesthetist should make those suggestions that will be most pleasing to this particular subject ... talk him to sleep, with the addition of as little ether as possible." In stomach cases, "as soon as the stomach is explored and the method of operation decide upon, the ether is withdrawn, the surgeon being able to continue operation, no more being given until time to close the incision ... thus we are able to complete the operation and avoid vomiting with an exceedingly small amount of anesthetic."
The Mayo brothers were well trained surgeons, but no more so than their peers at at Johns Hopkins and Harvard. Why did hundreds trek to remote Rochester, Minnesota ("You can't get there from here")? Because their anesthesiologist was named Alice Magaw, and you didn't die!
These clinical results are confirmed by more tightly controlled laboratory studies.
 In
In  the laboratory, the effect of
analgesia was demonstrated in a psychophysical study by Hilgard
(1967). subjects classified as
low, medium or high in hypnotizability (the last group including
some "virtuosos") were exposed to 60 seconds
of cold-pressor pain by submerging their hand
and forearm into circulating
ice-water. In this laboratory analog of clinical
pain, the pain mounts fairly quickly.
The subjects gave pain reports on an
open-ended 1-10 scale (meaning that they could use
numbers higher than 10) both with and without
suggestions for analgesia. The suggestions had
little effect on the insusceptible
subjects, and a little more effect on those of moderate hypnotizability, but reduced
felt pain by half in highly hypnotizable subjects. The
illustration at right shows a typical cold-pressor apparatus.
the laboratory, the effect of
analgesia was demonstrated in a psychophysical study by Hilgard
(1967). subjects classified as
low, medium or high in hypnotizability (the last group including
some "virtuosos") were exposed to 60 seconds
of cold-pressor pain by submerging their hand
and forearm into circulating
ice-water. In this laboratory analog of clinical
pain, the pain mounts fairly quickly.
The subjects gave pain reports on an
open-ended 1-10 scale (meaning that they could use
numbers higher than 10) both with and without
suggestions for analgesia. The suggestions had
little effect on the insusceptible
subjects, and a little more effect on those of moderate hypnotizability, but reduced
felt pain by half in highly hypnotizable subjects. The
illustration at right shows a typical cold-pressor apparatus.
 Pain
Pain  has two components, sensory pain (providing information about
the location and severity of irritation or injury), and
suffering (a psychological reaction depending on the meaning of
the sensory pain). Hypnotic analgesia alters both the qualia
associated with sensory pain and the intentionality associated
with suffering.
has two components, sensory pain (providing information about
the location and severity of irritation or injury), and
suffering (a psychological reaction depending on the meaning of
the sensory pain). Hypnotic analgesia alters both the qualia
associated with sensory pain and the intentionality associated
with suffering.
 An absolutely spartan study by Stern et al.
(1977) compared hypnotic analgesia with a number of other
"pain-challenging" treatments, including true
acupuncture (with electrical stimulation of the
acupuncture needles), placebo acupuncture, morphine, aspirin,
diazepam, and placebo pill. Hypnotizable subjects were
exposed to both cold-pressor and ischemic muscle pain under both
experimental and control conditions for each of the challenging agents. So, if you're doing the
multiplication, that's 2 (experimental vs. control) x 2
(cold-pressor vs. ischemia) x 7 (challenging agents) = 28 pain
trials per subject!
An absolutely spartan study by Stern et al.
(1977) compared hypnotic analgesia with a number of other
"pain-challenging" treatments, including true
acupuncture (with electrical stimulation of the
acupuncture needles), placebo acupuncture, morphine, aspirin,
diazepam, and placebo pill. Hypnotizable subjects were
exposed to both cold-pressor and ischemic muscle pain under both
experimental and control conditions for each of the challenging agents. So, if you're doing the
multiplication, that's 2 (experimental vs. control) x 2
(cold-pressor vs. ischemia) x 7 (challenging agents) = 28 pain
trials per subject!
 |
 |
 Other laboratory studies indicated that
hypnosis does not act as a tranquilizer or as a placebo.
Other laboratory studies indicated that
hypnosis does not act as a tranquilizer or as a placebo.
Hypnotic analgesia is not reversed by naloxone, an opiate antagonist, so it is not mediated by the release of endogenous opiates (endorphins).
With respect to the psychological mechanisms underlying hypnotic analgesia, most attention has focused Hilgard's proposal that analgesia is mediated by an amnesia-like dissociative barrier which diminishes the subject's conscious perception (awareness) of pain. Some evidence for this dissociative process comes in the form of Hilgard's studies of the "hidden observer", which revealed a persisting subconscious representation of pain, as well as observations that hypnotic analgesia does not alter psychophysiological responses to the pain stimulus. Based on this evidence, it appears that hypnotic analgesia alters the explicit but not the implicit perception of pain, just as posthypnotic amnesia alters explicit but not implicit memory.
In opposition to this dissociative view, Spanos has proposed that hypnotic subjects engage in stress inoculation procedures, such as self-distraction and recoding, which alter the subject's response to, but not his/her awareness of, the pain stimulus.
A series of studies by K.S. Bowers attempted to determine whether hypnotic analgesia is mediated by stress-inoculation strategies of the sort proposed by Spanos.
 Miller and Bowers (1986) found that subjects administered
hypnotic suggestions for analgesia did not report engaging in
stress inoculation strategies. Moreover, response to hypnotic
analgesia suggestions was mediated by hypnotizability, while
response to stress-inoculation instructions was not.
Miller and Bowers (1986) found that subjects administered
hypnotic suggestions for analgesia did not report engaging in
stress inoculation strategies. Moreover, response to hypnotic
analgesia suggestions was mediated by hypnotizability, while
response to stress-inoculation instructions was not.
 A second paper by Miller and Bowers (1993) showed that strategic
stress inoculation interfered with performance on a difficult
vocabulary test, while hypnotic analgesia did not.
A second paper by Miller and Bowers (1993) showed that strategic
stress inoculation interfered with performance on a difficult
vocabulary test, while hypnotic analgesia did not.
 Hargadon, Bowers, and Woody (1995) showed
that the use of counter-pain imagery, a common stress
inoculation strategy, had no effect on hypnotic analgesia. Taken
together, these studies show that stress inoculation can reduce
pain, but it does not mediate pain reduction in hypnotic
analgesia.
Hargadon, Bowers, and Woody (1995) showed
that the use of counter-pain imagery, a common stress
inoculation strategy, had no effect on hypnotic analgesia. Taken
together, these studies show that stress inoculation can reduce
pain, but it does not mediate pain reduction in hypnotic
analgesia.
Posthypnotic amnesia is so central to the experience of hypnosis that it gave the state its name. However, it does not occur unless it is suggested to the subject (directly or by implication), so it is not an instance of "state-dependent" memory.
On t he
standardized hypnotizability scales, such as the
Stanford Form C, the suggestion for amnesia
is administered toward the end of the scale, and covers
the other suggestions that were administered during testing (including the suggestion for
posthypnotic amnesia, if there is one).
Suggestions for amnesia always
include the arrangement for a
signal, known as a reversibility cue, to
cancel the amnesia suggestion. Compared
to insusceptible subjects,
hypnotizable subjects perform relatively poorly on tests of
free recall (Rl) and recognition (Rn) while the amnesia
suggestion is in effect. But they
perform normally on a test of free recall after the
amnesia suggestion has been canceled by the reversibility
cue. Reversibility makes
clear that posthypnotic amnesia reflects
a disruption of memory retrieval, as opposed to encoding
or storage. And because the
subjects are wide awake during both
initial amnesia and reversibility, reversibility
confirms that posthypnotic amnesia is not a reflection of state-dependent memory.
he
standardized hypnotizability scales, such as the
Stanford Form C, the suggestion for amnesia
is administered toward the end of the scale, and covers
the other suggestions that were administered during testing (including the suggestion for
posthypnotic amnesia, if there is one).
Suggestions for amnesia always
include the arrangement for a
signal, known as a reversibility cue, to
cancel the amnesia suggestion. Compared
to insusceptible subjects,
hypnotizable subjects perform relatively poorly on tests of
free recall (Rl) and recognition (Rn) while the amnesia
suggestion is in effect. But they
perform normally on a test of free recall after the
amnesia suggestion has been canceled by the reversibility
cue. Reversibility makes
clear that posthypnotic amnesia reflects
a disruption of memory retrieval, as opposed to encoding
or storage. And because the
subjects are wide awake during both
initial amnesia and reversibility, reversibility
confirms that posthypnotic amnesia is not a reflection of state-dependent memory.
Explicit and Implicit Memory in Posthypnotic Amnesia
 In
In  the laboratory, posthypnotic amnesia is usually
studied by giving subjects a list of words to study, or
memorize, while they are hypnotized.
Then the subjects receive a suggestion that they will
forget what they did or experienced during hypnosis,
including the learning experience, until the hypnotist gives the reversibility cue.
the laboratory, posthypnotic amnesia is usually
studied by giving subjects a list of words to study, or
memorize, while they are hypnotized.
Then the subjects receive a suggestion that they will
forget what they did or experienced during hypnosis,
including the learning experience, until the hypnotist gives the reversibility cue.
A pair of studies from my laboratory showed that posthypnotic
amnesia impairs explicit memory, as reflected in recall or
recognition, but spares implicit memory, as reflected in priming
effects on free association or category generation.
In
Experiment 1, subjects memorized a list containing words like girl, chair, flowers, and short under hypnosis, and then received suggestions for posthypnotic amnesia. The virtuoso subjects were unable to recall the list items, showing the predicted impairment in explicit memory. Later, they were asked to free-associate to "critical" stimuli such as boy, table, blossom, and long, which were intended to target the studied words as free associates; they also free-associated to other, "neutral", words, such as lamp (light), dogs (cats), and man (woman), which did not target the memorized items. Subjects were more likely to give the targeted responses to "critical" vs. "neutral" stimuli, showing a priming effect. But the magnitude of the priming effect did not differ between the hypnotizable subjects, who were amnesic for the critical targets, and the insusceptible subjects, who were not amnesic.
In both experiments, posthypnotic amnesia impaired explicit memory, in the form of free recall, but spared implicit memory, as reflected in priming on the free-association or category-generation tasks. And in both cases, the preserved priming was semantic in nature -- not merely repetition priming.
Experiment 2 had exactly the same format, except it employed a different test of implicit memory. This time, the subjects memorized a list containing instances of various conceptual categories, such as Judy, foot, lion, and day. For the implicit memory test, the subjects were asked to generate instances of "critical" categories, such as woman's name, body part, animal, and period of time; there were also "neutral" categories, such as man's name, country, article of clothing, and color. Again, the virtuoso subjects, who were densely amnesic on a test of free recall, showed priming effects that were the equivalent to those shown by the insusceptible, non-amnesic subjects.
 A
A
 more
recent
followup study by Jennifer Dorfman confirmed
these essential results.
more
recent
followup study by Jennifer Dorfman confirmed
these essential results.
 Another study, by Barnier et al. (2001), compared
repetition and semantic priming. As usual, the
subjects studied a word list in hypnosis, followed by an amnesia suggestion. then the
subjects were given a cued-recall test of explicit
memory, followed by fragment
completion test of repetition priming and a
word-association test of semantic priming. As
expected, the hypnotizable subjects showed amnesia on
the cued-recall test of explicit memory; but compared to
baseline levels, both the insusceptible/nonamnesic and
the hypnotizable/amnesic subjects
showed significant priming on both tests of implicit
memory.
Another study, by Barnier et al. (2001), compared
repetition and semantic priming. As usual, the
subjects studied a word list in hypnosis, followed by an amnesia suggestion. then the
subjects were given a cued-recall test of explicit
memory, followed by fragment
completion test of repetition priming and a
word-association test of semantic priming. As
expected, the hypnotizable subjects showed amnesia on
the cued-recall test of explicit memory; but compared to
baseline levels, both the insusceptible/nonamnesic and
the hypnotizable/amnesic subjects
showed significant priming on both tests of implicit
memory.
 In another study, David et al. (2000)
applied a variant of Jacoby's Process-Dissociation Procedure to
posthypnotic amnesia. The subjects studied the usual sort of word-list, followed
by an amnesic suggestion, and then completed a
stem-cued recall test of explicit memory and
a stem-completion test of implicit memory. In their
variant on PDP, they were able to decompose stem-completion
performance into three components: voluntary conscious memory
-- essentially explicit memory; involuntary
conscious memory, in which the cue automatically brought
a word to mind which was subsequently recognized as a list
item; and involuntary unconscious memory, essentially
implicit memory. Compared to insusceptible subjects, the
hypnotizable subjects showed a profound deficit on both measures of
conscious, explicit memory (both voluntary and
involuntary; but performed equally on the measure of
involuntary, unconscious, implicit memory.
In another study, David et al. (2000)
applied a variant of Jacoby's Process-Dissociation Procedure to
posthypnotic amnesia. The subjects studied the usual sort of word-list, followed
by an amnesic suggestion, and then completed a
stem-cued recall test of explicit memory and
a stem-completion test of implicit memory. In their
variant on PDP, they were able to decompose stem-completion
performance into three components: voluntary conscious memory
-- essentially explicit memory; involuntary
conscious memory, in which the cue automatically brought
a word to mind which was subsequently recognized as a list
item; and involuntary unconscious memory, essentially
implicit memory. Compared to insusceptible subjects, the
hypnotizable subjects showed a profound deficit on both measures of
conscious, explicit memory (both voluntary and
involuntary; but performed equally on the measure of
involuntary, unconscious, implicit memory.
The dissociation between explicit and implicit memory observed in posthypnotic amnesia resembles those discussed earlier, in the lectures on Explicit and Implicit Cognition, in cases of the amnesic syndrome or electroconvulsive therapy. However, the dissociation observed in hypnosis differs from that observed in other forms of amnesia: the memories lost were deeply processed at the time of encoding; the preserved priming is semantic rather than perceptual in nature; and the amnesia is reversible. Reversibility marks posthypnotic amnesia as a disorder of memory retrieval, rather than of encoding or storage.
Hypnotic Agnosia
 Posthypnotic
amnesia is a disruption in episodic memory, but there is also
some provisional evidence for hypnotic agnosia,
involving disruptions in semantic memory. Whereas posthypnotic
amnesia spares priming in free association, hypnotic agnosia
appears to impair free associations.
Posthypnotic
amnesia is a disruption in episodic memory, but there is also
some provisional evidence for hypnotic agnosia,
involving disruptions in semantic memory. Whereas posthypnotic
amnesia spares priming in free association, hypnotic agnosia
appears to impair free associations.
Hypnotic Hypermnesia?
Although hypnotic amnesia and agnosia appear to impair conscious awareness of memory, it has also been claimed that hypnotic suggestions can restore conscious access to memories which have been lost due to repression, dissociation, or even ordinary forgetting. However, clinical folklore about the effectiveness of hypnotic hypermnesia has not been validated by appropriately controlled laboratory and clinical studies. Hypnosis adds nothing to the hypermnesia observed with repeated recall trials in the normal waking state, even among highly hypnotizable subjects. Following hypnotic suggestions for hypermnesia, the bulk of new items remembered are false rather than accurate. When waking recall is retested in hypnosis, subjects tend to promote guesses to confident memories, and appear more responsive to leading questions. In summary, the evidence indicates that hypnosis exaggerates false recollection, increasing the frequency of false alarms but not of hits, and it also inappropriately increases the subjects' confidence in their memories, regardless of whether these memories are true or false. These results from laboratory studies are supported by more "real-life" experiments involving memory for staged crimes and comparisons of hypnotic and nonhypnotic techniques with actual witnesses and victims. Hypnotic hypermnesia is the illusion of enhanced memory.
Another illusory alteration of memory is hypnotic age regression, where the subjects receive suggestions to return to a previous time in their lives (or, in some cases, to previous lives!). Although some subjects respond to such suggestions with displays of childlike behavior, there is no evidence that age regression actually entails a psychological return to childhood, as measured by ablation (the loss of adult declarative and procedural knowledge), reinstatement (the return to archaic modes of cognitive and emotional functioning), or revivification (the restoration of forgotten memories of childhood). Hypnotic age regression, like hypnotic hypermnesia, is illusory.
The illusory nature of hypermnesia and age regression indicates that these techniques are not suitable for refreshing memories of witnesses and victims in forensic situations; nor are they recommended for recovering memories of trauma and other experiences of childhood. In the absence of independent corroboration, no credibility should be attached to any memory "recovered" by means of hypnosis; hypnotically recovered memories should be considered to be inherently unreliable.
Just as hypnotic suggestion can alter conscious memory, so it can alter conscious perception. The hypnotic effects on perception take four forms: positive hallucinations (where the subject perceives some object not actually present in the environment); negative hallucinations (where the subject fails to perceive an object that is actually present); anesthesias (reduction in acuity in some sensory modality), and hyperesthesia (enhanced acuity). With the exception of some provocative evidence for improved visual acuity in myopic subjects, the effects of suggestions for hyperesthesia, like suggestions for hypermnesia, appear to be illusory.
 Priming has also
been used to reveal implicit perception in hypnotic blindness.
In one study, subjects were given hypnotic suggestions for
blindness, and then presented with cards on which were printed a
homophone and a disambiguating cue word (e.g., war-peace).
The subjects were unable to recall the words that had been
presented to them, providing prima facie evidence of
blindness (you can't consciously recall an event you didn't
consciously perceive!). Nevertheless, when administered a
spelling test including both "seen" and "unseen" homophones,
they showed a strong tendency to spell the homophones in
accordance with the way they were presented (e.g., peace
rather than piece).
Priming has also
been used to reveal implicit perception in hypnotic blindness.
In one study, subjects were given hypnotic suggestions for
blindness, and then presented with cards on which were printed a
homophone and a disambiguating cue word (e.g., war-peace).
The subjects were unable to recall the words that had been
presented to them, providing prima facie evidence of
blindness (you can't consciously recall an event you didn't
consciously perceive!). Nevertheless, when administered a
spelling test including both "seen" and "unseen" homophones,
they showed a strong tendency to spell the homophones in
accordance with the way they were presented (e.g., peace
rather than piece).
 Suggestions
can be given during hypnosis for behaviors that will be executed
outside hypnosis, in response to a cue. These posthypnotic
responses appear to be automatic, but they do not fulfill the
standard criteria for automaticity.
Suggestions
can be given during hypnosis for behaviors that will be executed
outside hypnosis, in response to a cue. These posthypnotic
responses appear to be automatic, but they do not fulfill the
standard criteria for automaticity.
Beyond pain control there are a number of interesting studies
of the "psychosomatic" effects of hypnotic suggestion. A classic
clinical study by Mason successfully used hypnotic suggestions
to relieve a case of congenital icthyosiform erythroderma of
Broq. Other studies indicate that hypnotic suggestion can
modulate allergic responses and accelerate the healing of burns.
Most systematic study has been devoted to the treatment of
warts. A number of well-controlled studies indicate that
suggestions can lead to the remission of warts, although the
operative factor appears to be suggestion, independent of
hypnosis. The psychosomatic effects of hypnotic and nonhypnotic
suggestion shed new light on the mind-body problem by showing
how one’s mental state (i.e., beliefs, images, and expectations)
can alter one’s physical state (e.g., allergic reactions or
warts). Some of these studies are discussed in the
lectures on Psychosomatic
Effects.
Brain-imaging studies of hypnosis have now begun to appear.
 One
One  study, by Rainville et al. (199&0,
used hypnotic suggestions to reduce and enhance the "suffering"
component of pain, leaving the "sensory" component unaffected.
PET imaging revealed that hypnotic modulation of suffering was
associated with changes in the anterior cingulate cortex,
leaving the primary sensory cortex unaffected. Apparently,
the primary sensory cortex mediates sensory pain, while the
anterior cingulate cortex mediates suffering.
study, by Rainville et al. (199&0,
used hypnotic suggestions to reduce and enhance the "suffering"
component of pain, leaving the "sensory" component unaffected.
PET imaging revealed that hypnotic modulation of suffering was
associated with changes in the anterior cingulate cortex,
leaving the primary sensory cortex unaffected. Apparently,
the primary sensory cortex mediates sensory pain, while the
anterior cingulate cortex mediates suffering.
 Another
Another  PET study, by Kosslyn et al. (2000),
showed that hypnotic modulation of color perception ("draining"
or "adding" color to a stimulus) affected activation in the
"fusiform color area" and the inferior temporal region of
cerebral cortex.
PET study, by Kosslyn et al. (2000),
showed that hypnotic modulation of color perception ("draining"
or "adding" color to a stimulus) affected activation in the
"fusiform color area" and the inferior temporal region of
cerebral cortex.
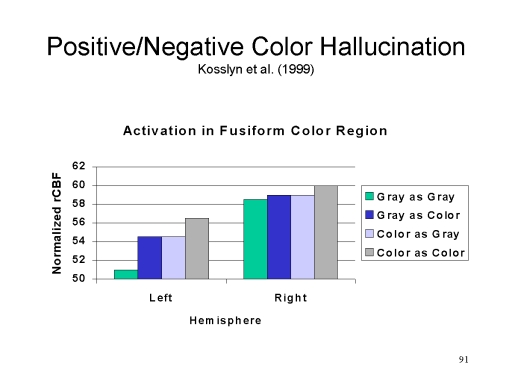 In
In  hypnosis,
perception of color, real or hallucinated, led to activation of
the fusiform color area, with the effects are clearer in the
left cerebral hemisphere than in the right. Somewhat
similar effects were observed in unhypnotized subjects who
received the same suggestion. It's the experience that
matters, not whether the subject was hypnotized. However,
activation in the left fusiform area was affected only during
hypnosis. The right fusiform activation was affected in
both the hypnotic and the control condition.
hypnosis,
perception of color, real or hallucinated, led to activation of
the fusiform color area, with the effects are clearer in the
left cerebral hemisphere than in the right. Somewhat
similar effects were observed in unhypnotized subjects who
received the same suggestion. It's the experience that
matters, not whether the subject was hypnotized. However,
activation in the left fusiform area was affected only during
hypnosis. The right fusiform activation was affected in
both the hypnotic and the control condition.
Studies of posthypnotic amnesia reveal a dissociation between explicit and implicit memory: amnesic subjects cannot consciously remember events that nonetheless continue to influence their behavior.
Similarly, hypnotic analgesia may serve to illustrate the dissociation between explicit and implicit perception. The subject is not aware of pain inflicted by the stimulus (an impairment of explicit perception), but studies of the hidden observer, and of psychophysiological responses to the pain stimulus, indicate that implicit perception of pain is spared.
Studies of hypnotic deafness, hypnotic blindness, and negative hallucinations also appear to illustrate the dissociation between explicit and implicit perception in the visual and auditory domains.
Taken together, these findings are consistent with the notion of an amnesia-like barrier which alters conscious awareness while permitting subconscious processing to continue, as suggested by Hilgard's neodissociation theory of divided consciousness.
This page last revised 08/17/2021.


